During symposium sponsored by Lilly, professor Thomas Danne, and experts, including Crystal Bowersox, patient, and expert, emphasize in the importance of diabetes education in hypoglycemia and the impact and consequences of severe hypoglycemia. There is a strong need for diabetes education and establishing personal glucose targets to prevent hypoglycemia. https://www.easd-industry.com/programme/from-science-to-reality-understanding-the-silent-side-of-severe-hypoglycemia
My main question is whether or not its MARD is better than the Libre 1. Given that the Dexcom G6 has an improved MARD over the G5, and that Abbott is working on a closed loop system with Bigfoot and want to use the Libre 2 in it, I think it is rather likely.
FreeStyle Libre has a MARD of 9.5% vs. YSI, with 90% of readings within ± 20%/20 mg/dl vs. YSI in adults and pediatrics (4-17 years) – the data is near-identical to the US 14-day version
Dr. James Gavin: Categorical “Treatment Boxes” Do Not Adequately Address the Heterogeneity and Diversity of Diabetes
In a riveting keynote lecture on the diversity and heterogeneity of diabetes, Emory University’s Dr. James Gavin advocated for a novel classification system to “illuminate the pathway to comprehensive, better-targeted, and more effective treatment of diabetes.”
Dr. Gavin criticized how, historically, diabetes has been classified into the narrow “treatment boxes” of type 1 (i.e. antibodies and beta cell destruction) vs. type 2 (i.e. insulin resistance). In his view, the beta cell destruction vs. insulin resistance framework is an oversimplification. He described how antibody positive patients can present as if they have type 2 diabetes, and how type 1 patients can present with insulin resistance (i.e., looking like type 2 diabetes). To parallel the oversimplified classification scheme for diabetes, Dr. Gavin argued that the standard framework for diabetes treatment is equally narrow: Insulin for type 1 diabetes and stepwise addition of oral anti-diabetic agents and eventually insulin for type 2 diabetes. He noted that although diabetes diagnoses may have extensive clinical overlap, differences in etiology, phenotype, and (likely) genotype are important further considerations to determine a more individualized treatment plan.
Dr. Gavin pointed out that the current glucose-centric diagnostic model for diabetes often “handcuffs” clinicians into solely focusing on reducing A1c without adequately addressing its causes or engaging with opportunities to attenuate comorbidities. To this end, he highlighted a new classification method that describes five subtypes within type 2 diabetes, and a beta cell centric model (the “egregious eleven”) which allows for tailored treatment of 11 specific pathways associated with diabetes at both the physiologic and genetic levels.
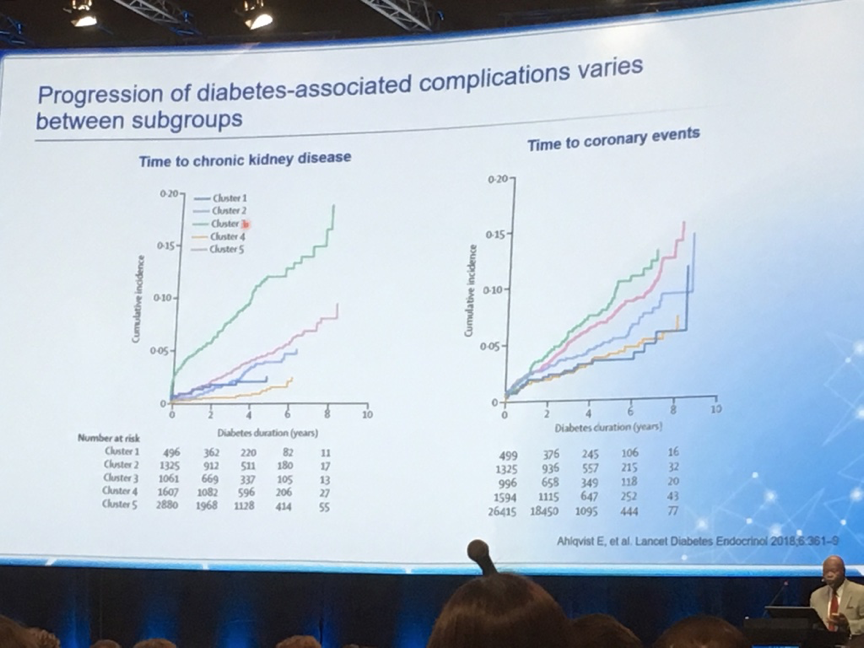
Dr. Gavin pointed to a 2018 Lancet study which created five “clusters” within type 2 diabetes: (1) Severe autoimmune diabetes (SAID); (2) Severe insulin-deficient diabetes (SIDD); (3) Severe insulin-resistant diabetes (SIRD); (4) Mild obesity-related diabetes (MOD); and (5) mild age-related diabetes (MARD) . These clusters are based on six clinical variables: (1) Glutamate decarboxylase antibodies (GADA); (2) age at diagnosis; (3) BMI; (4) A1c; and homoeostatic model assessment estimates of (5) beta cell function and (6) insulin resistance. Lending credence to the idea of distinct subtypes within type 2 diabetes is the observation that these cohorts experience very different rates of progression of diabetes-associated complications (see below). Furthermore, there are genetic differences between the cohorts. For instance, a variant in the TCF7L2 gene (previously thought to be associated with type 2 diabetes in general) was associated with SIDD, MOD, and MARD but not SIRD. Importantly, carriers of this TCF7L2 risk-variant do not respond to incretin therapy (e.g., GLP-1 agonists), so SGLT-2 inhibitors or insulin are a better option for A1c reduction. As such, there is significant potential to leverage the heterogeneity of type 2 diabetes into more individualized, effective therapies (we’re nervous to say “precision medicine” as this has become a buzzword, though this is certainly a step closer to that coveted level of personalization). Dr. Gavin pointed out that not only would this confer better patient outcomes, but would also help avoid unnecessary patient/provider frustration over a less-than-ideal response to an initial prescription (e.g. a GLP-1 agonist for a TCF7L2 risk-variant-carrying patient). This frustration is all too common with the current treat-to-fail paradigm of diabetes prescriptions.
Dr. Gavin argued that diabetes is even more nuanced than the famous “ominous octet” would suggest, describing an alternative “egregious eleven” which includes the influence of the microbiome, immune system, and increased glucose absorption in the stomach and small intestine in addition to the traditional players – impaired insulin secretion in the beta cells, increased glucagon secretion in the alpha cells, increased hepatic glucose production, neurotransmitter dysfunction, decreased muscular glucose uptake, increased glucose reabsorption in the kidneys, increased lipolysis in adipose tissue, and a decreased incretin effect in the gut. He argued that factors within the egregious eleven are selectively treatable (or likely to be treatable in the future), making possible a targeted and individually-tailored diabetes treatment plan, depending on a patient’s particular pathophysiology. Taking this one step further, Dr. Gavin emphasized that well-designed, early combination regimens have the potential to address most defects concomitantly – a major win for patients and vote of confidence in up-and-coming dual- and tri-agonists, such as GLP-1/GIP and GLP-1/glucagon agonists, that target multiple aspects of the egregious eleven.
To conclude, Dr. Gavin touched on the value of real-world evidence to complement and expand upon existing RCTs. He argued that management of a disease as complex and heterogeneous as diabetes depends on many factors that we don’t (or can’t) measure in RCTs. RWE therefore represents perhaps the only way we can get insight into critical issues such as patient preferences, likelihood of adherence, impact of cost, and complexity of certain treatment regimens.
PIONEER 1 trial indicated that, in comparison with placebo, once-daily oral semaglutide was associated with significant reductions in HbA1c, weight and both in adults with type 2 diabetes.
Professor Jaakko Tuomilehto “Early weightloss predicts greater type 2 diabetes prevention effect” lifestyle early interventions seem to have predictive success.
Roche and Novo Nordisk will work together to integrate insulin dosage information from Novo Nordisk’s connected pen technology into Roche’s open ecosystem, communicating with its digital diabetes management solutions including mySugr, according to Press Release
New European Diabetes Forum launched to drive policy the European Association for the Study of Diabetes (EASD) has announced the launch of a new coalition, the European Diabetes Forum (EUDF). The Forum’s Call to Action sets out the identified causes in European healthcare systems of the failure in managing a chronic, complex and growing disease like diabetes, as well as potential solutions to address them.