Your summary sounds partially true and partially confused with Medtronic and Omnipod 5. A lot of the information you’re asking about is not actually detailed at all, but can be answered just by looking at Tandem’s website, or by reading the quick facts sheets and/or the user manual.
Control-IQ is nearly entirely based off of your own personal basal profile(s) settings, for better or worse. Simply put, the better your settings, the better your medical support team and/or the better you understand how to adjust pump settings, the better your outcome. Assuming your desired outcome aligns with the Control-IQ targets! The most critical settings are correction factor (same as ISF) and the programmed basal rate(s).
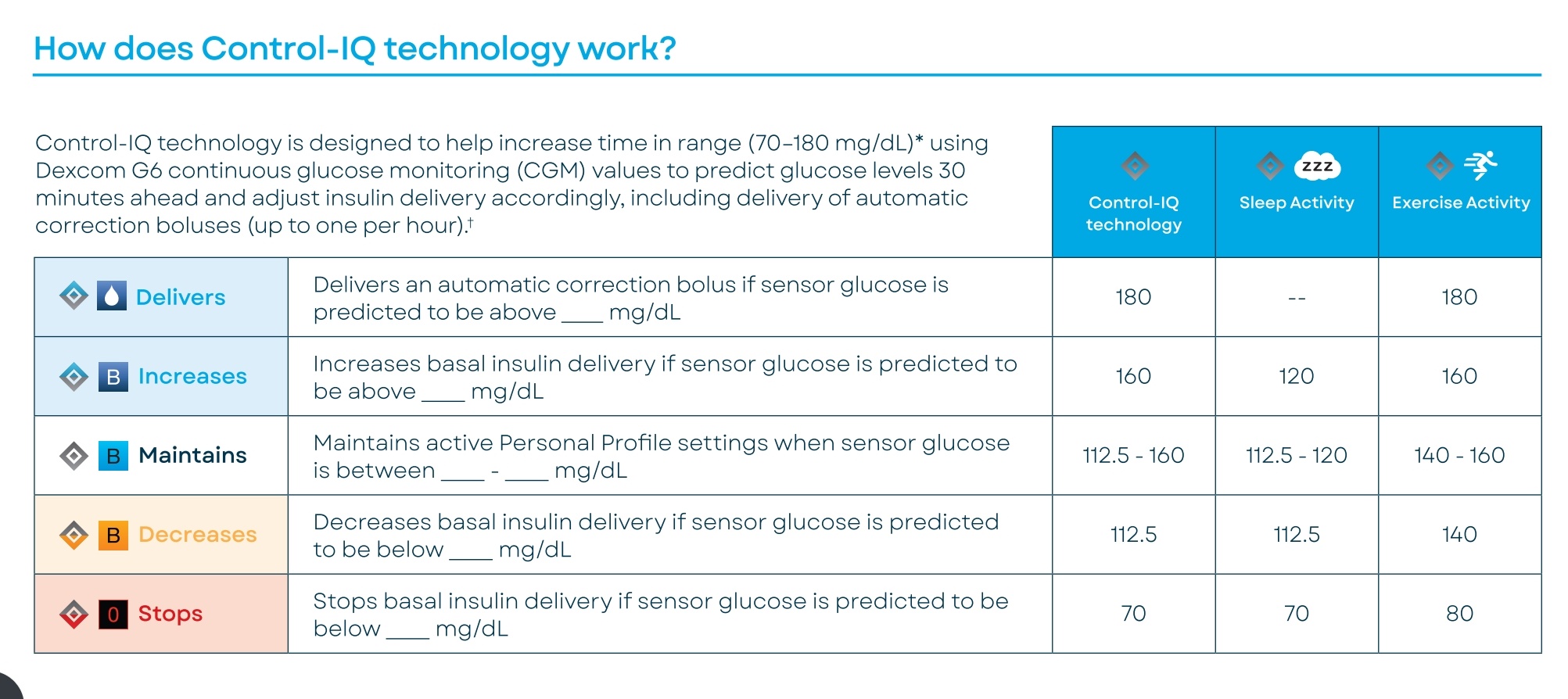
Control-IQ works off of actionable ranges, based on where Dexcom predicts you will be in 30 minutes. Your current BG matters little. There are three different programs of actionable ranges to choose from. Within each program, there is a target zone, in which Control-IQ does absolutely nothing and your programmed settings are allowed to run without intervention. If you’re predicted to stray slightly outside the target range, it will either reduce or increase your basal rate, informed by your correction factor. If you’re predicted to go to an extreme, then you get extreme intervention… Either by means of an automatic correction bolus (only 60‰ of the calculated dose as a safety measure, and the calculated does does indeed account for IOB), or a complete insulin suspension at the other end of the spectrum.
It sounds like you’ve already seen this chart, or at least one similar to it, but maybe didn’t fully understand it? This is literally how Control-IQ works. When it talks about increasing or decreasing basal rates, it’s doing so to the basal rate you programmed, not to one it manufactured based on your weight and TDD.
Speaking of weight and TDD… You will have to enter these values when you first set up Control-IQ, but your total daily dose will quickly be substituted with actual data from your pump’s history. This is the ONE AND ONLY bit of “learning” Control-IQ does. Unlike other systems, these are not used to determine insulin DELIVERY, but rather the exact opposite. They’re used to impose safety limitations on the system, which will override any extreme value the system might otherwise deliver. (This information is in the manual.) Control-IQ knows that someone who weighs 80 lbs and only takes 20 units a day is much more sensitive to insulin than someone who weighs 200 lbs and takes 100 units in a day, so Control-IQ is much less aggressive with that more sensitive individual.
Your programmed basal rate is also really critical to get the correct IOB to display. The IOB is calculated as a net value. it only displays whatever insulin on board is in addition to your basal rate. If it withholds any insulin, it is subtracted from the IOB (the excess insulin you had on board is essentially redirected to be used as basal instead). If it gives any additional insulin, it adds it to the IOB, as we would expect. If your programmed basal rate isn’t true, though, it will negatively reflect in your IOB. If your basal rate is set too high, excess insulin on board will be hidden from you and Control-IQ. If it’s set too low, it will look like you have more insulin on board than is actually true. Since IOB is used to inform the choices Control-IQ makes, basal testing is HIGHLY recommended.
If this isn’t enough and you want to go further down the rabbit hole and really get detailed information about how Control-IQ works… You won’t find everything in one place, but you can piece together a lot of information from multiple sources to get a bigger picture.
Tandem partnered with Type Zero to formulate Control-IQ. Type Zero’s automatic insulin dosing algorithm was based off of years of research coming out of the University of Virginia. You can learn a lot about how Control-IQ works now by looking at that original research. One of the greatest contributions of that original research was a brand-new insulin decay model, that is unlike anything else ever used before in a commercial pump system. It more accurately reflects the true 5 hour long action curve of our analog insulins. All other pumps, and even the T:slim X2 when Control-IQ is disabled, use what is known a “curvilinear” model, which can only encorporate the steepest segment of the insulin action curve. This is why Control-IQ has the DIA locked in at 5 hours, instead of the usual 2.5-4 hours users might be accustomed to. That standard curvilinear model is very much like trying to fit a round peg into a square hole. It just doesn’t match real insulin action well, and the users basically has to decide how much of the lingering tail they feel comfortable ignoring. Control-IQ uses the full picture, though, to better account for the potential impact of all IOB
I seem to recall an interesting discussion about this by Stacey Simms on her Juicebox Diabetes Connection (edited) podcast. I believe it was the episode in which she discussed why her family switched to Control-IQ instead of continuing with DIY closed loop for her T1 son. In fact, she’s been a great source of more detailed information since she’s done several interviews with Tandem employees who have insider knowledge.
If you navigate to the Tandem diabetes webpage, then choose the “providers” tab, you’ll find much more involved information than on the patient side of things. They even share all the clinical research, which contain commentary on the algorithm workings.
And even farther down the rabbit hole yet… They give their investors, or potential investors, way more information than they share elsewhere with the patients. They share the exciting science advancements add a way to entice new investors. I’ve been stalking every investor update for years for exactly this reason. There’s a financials website called Motley Fool, which posts text transcripts of all the back meetings. You can search as far back as 2017 for Control-IQ information.