I’m an outlier here- an engineer with 40 years experience with T1D. I’m skeptical about complex technology reliability but more skeptical about anything that is simple technologically being a larger cause of application failures than human factors.
This tech is less complex than a cellphone, simpler than a programmable thermostat and a heat pump system. Instead of keeping the indoor temperature in a comfortable range by cycling between chill/idle/heat, it tries to keep glucose within a comfortable range by cycling a insulin pump on and off. It’s smaller with a glitzier UI, but it’s not new technology, just repackaging.
A CGM sensor is a wire with a coating that uses the same kind of electrochemical reaction as a blood glucose meter. The “transmitter” is a one or two chip integrated AD converter and BT transmitter. The probability of either being defective as shipped is much less than 1%. Both are simple enough to be tested 100% before shipping, and are. They can be damaged during transit by extreme, prolonged heat or cold
In comparison, the probability of a skin site everr being bruised, bleeding, or scarred in the interstitial layer or an inserted wire being moved within the interstial layer after insertion is much greater. Insulin flow is a larger molecule than glucose. Except for being slower, insulin flow in the interstitial layer to capillaries for basal delivery is nearly identical to glucose flow from capillaries to sensor wires. Glucose has the easier job.
I’ve done MDI +3x/day on average for 44 years. I know that I have injection sites that work poorly and I automatically avoided them or used longer or shorter needles - until I started using a CGM and pump and temporarly forgot what I learned. Once I remembered, I was able to start systematically mapping out my good sites, using this chart. https://usercontent.one/wp/www.bubblan.org/wp-content/uploads/2021/08/ijectionsites.png?media=1670715774
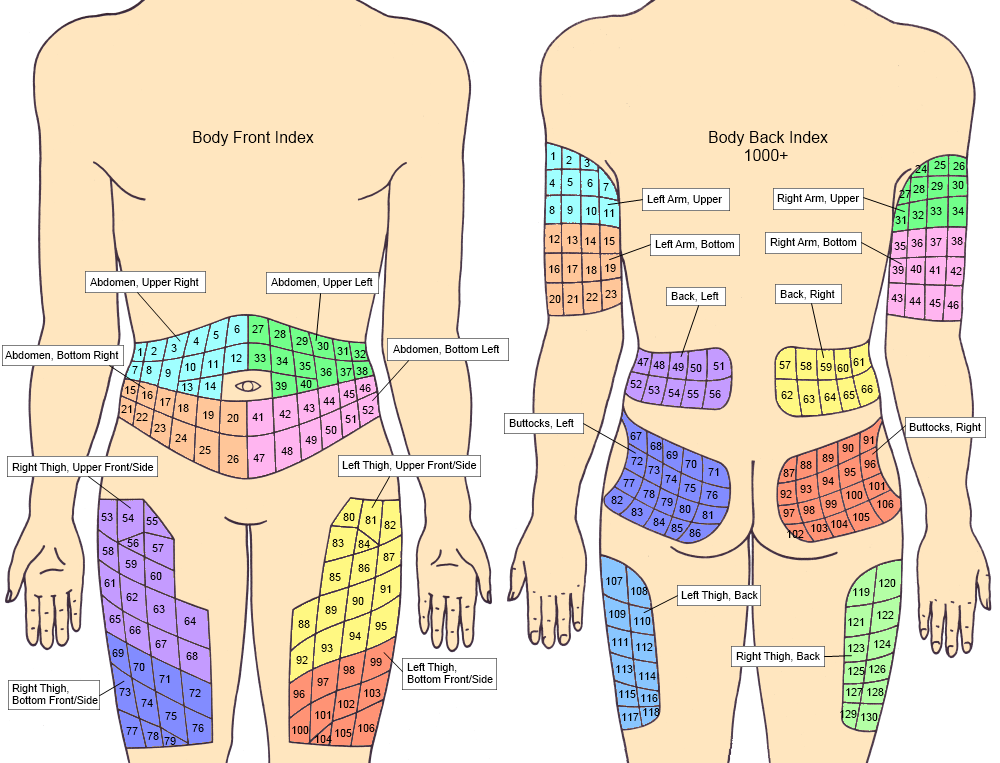{kind=link}
I had a much higher failure rate with plastic cannulas than with steel even though I utilized secondary strain relief. The steel cannulas eliminated one variable. If I had a “bad infusion site” I could move the cannula to the last known good site. Invariably the relocated system worked normally. Nearly every time I’ve used a known good infusion site for CGM sensor placement, it has been problem-free.
My experience suggests that the plastic cannula is more likely to cause or encounter underskin trauma than steel, and the thinner sensor wire has an easier time penetrating to an area clear of fluid resistance than either cannula.
I’ve used every kind of tool available for managing BG, delaying the adoption of each until I saw solid evidence that it not only “worked”, but was cost effective AND improved outcomes. AFAIC if a tech doesn’t increase my lifespan and make my QOL better, it’s worthless. Only one new tech has proven to be measureably effective in improving outcomes since 1980. It’s not “better” insulin, not pumps. It’s CGMs.
An insulin pump has an order of magnitude more mechancal complexity than a CGM and two orders of magnitude more electronic complexity. So I spent time more testing a Tandem pump manually, with Basal IQ and Control IQ software, than I did CGM sensors. The one I have is as reliable as my cellphone. All it lacks, imo, is a simple way to do a factory reset. The closest equivalent is to apply a software update. The next closest is like resetting a browser - disable the IQ software, create a new profile, power it off and on, and re-enable the IQ software.
My conclusion is that if I want excellent BG control, I test every site, infusion and CGM, for proper operation, and I look at to the readings before mealtime, neither a malfunctioning CGM nor the pump can prevent me from maintaining excellent control.
Knowing how to manually manage my BG based on glucose readings, but not doing it, will.