I have struggled with my weight my whole life, and I believe it can largely be related to my Diabetes. I was diagnosed when I was 2 1/2 and had my fair share of lows & seizures growing up as my parents and I learned to get a handle on the disease. My mother developed (and I believe instilled in me, not to blame her for protecting me!) a fear of lows, and so I began over correcting my lows, and eventually, over eating,
All that to say, I am changing my life style this year, and have lost about 24 pounds in 6 months. Not rapid, but I’m working on making sustainable lifestyle choices that I can keep up with, without starving myself and feeling malnourished (like I have in weight loss binges in the past, losing 20+ pounds over the course of a month).
So, circling back to my Topic title, what are some good snack suggestions to correct a low with, without stacking on the calories? I work out regularly, and experience lows while working out, and usually throughout the night. I’m trying to catch the cycle to update my basal, but haven’t had success yet. Let me know your thoughts, sorry for the rant & life story!
I use glucose tablets because of the precision they offer. I know exactly how many carbs I’m getting and can tailor the dose to my meter reading.
That said, many people dislike the tablets because of taste or whatever. I don’t mind them in the slightest, so I guess I’m one of the lucky ones that way.
For the lows while exercising, if you can share a little information, I can point you in the right direction. Are you on a pump, or are you using a basal insulin injection?
If you are using basal injections, can you tell me which insulin you are using for that and the timing of your injections and the timing of your workouts? It can be done with MDI or pump, but MDI is a bit trickier.
For the lows at night, I know how much exercise can affect that. Sometimes 50% basal reduction for me just from exercise. Are you doing low carb?
And for the weight loss, tell me what type of exercise you are doing. Do you use heart rates for that?
I use Omni Pod & a Dexcom G5 Cgm (only as of about a month ago, so getting used to both).
Yes to low carb and calories. I’m finding almost all of my daily calories are coming from my low corrections. I currently utilize the glucose tabs and juice boxes, depending where I’m at when the low occurs (always keep two juice boxes on my bedside table, as often times I will have more than one low per night after I’ve exercised).
I do a bit of everything for exercising, I do wear a fit bit and my end goal is to get my heart rate up to my fat burning zone. Usually Cardio intensive.
I also like glucose tablets for their calibrated precision. The standard medical advice encourages eating 15 grams of carbs when low, waiting 15 minutes, measuring your blood glucose again, and repeat if needed.
I have two problems with this general advice. My first caution when following this protocol concerns over-treatment. All lows are not created equal. Is it a hard charging low that is dropping fast with some insulin on board (previous dose, yet to act) or is it a slowly dropping blood glucose (BG) with little to no insulin on board? A calibrated response geared to your body’s actual needs is much better than the shot-gun approach often given.
My second point is the level at which you start to treat your hypoglycemia. I remember being told to correct anything under 80 mg/dL (4.4 mmol/L). For me, this threshold of treating low BGs causes needless calorie consumption and drives up detrimental BG variability. Over the years I’ve found that my body starts to counter-regulate with adrenaline at about 65 mg/dL (3.6 mmol/L). So this is my personal action threshold; yours may be different.
I find following my continuous glucose monitor (CGM) is valuable to me whether to treat a hypo, let it ride, or even to treat aggressively. I will often treat hypos with as little as 1/2 of 1 glucose tablet. If you don’t use a CGM and have the option to get one, I would give it consideration.
Congrats on your weight loss! I’ve lost some weight recently and I find it invigorating.
I have written a number of things about this on another site, but many of those lows you are having at night are from your body replacing the muscle glycogen you use when you are exercising.
Your body has 3 main fuel tanks it uses - glucose stored as muscle glycogen, fatty acids stored as triglycerides, and muscle protein (amino acids).
When you use your muscle glycogen, your body replaces it later in the day. It pulls from your blood sugar to refill the muscle glycogen tank. That can cause you to drop at night. The trick to avoid that is to replace the muscle glycogen immediately after exercise!
When you try to get in the fat burning zone, what numbers are you using for heart rate? Have you calculated the right HR rate?
Generally you will be burning some muscle glycogen and some fat during cardio. How much of each depends on the intensity and your condition.
With pods it is super easy to do basal adjustments to help during exercise.
Also, a commonly accepted but somewhat undocumented thought in the running community, is that caffeine helps your body gear more toward fat metabolism instead of muscle glycogen…
Another vote for glucose tabs. For me, they are the fastest-acting, easiest to control and … “utilizes the least amount of calories” (16 calories/tab).
Since you’re on a pump and using a CGM, I would urge you to experiment with temporary basal rates (TBRs). TBRs are really key to being able exercise an minimize going low. I like to start a lower TBR at least 1 hour before exercise. I also will use a lower TBR overnight.
@Eric2 - great info. How do you replace muscle glycogen immediately after exercise?
Apart from using glucose tabs if you are actually hypo, the most effective way is to try to avoid hypos by anticipating them. This really only works if you are using a pump plus either CGM or Flash monitoring. If your levels are falling and you have active insulin (Bolus insulin) on board, you should be able to predict using your insulin sensitivity factor (ISF) if the trend is going to take you below your lower limit. If so, my strategy is to do what an Artificial Pancreas program would do and cut basal to zero for long enough to compensate for the excess IOB. It is important to do this in advance. Even if my current sensor reading is above target, I will apply a 30 or 60 minute temporary basal of minus 90 or 100 perecnt. This strategy means that the hypo will probably never happen.
Example:
Current sensor 6.9 and falling slowly (no down arrow). Active IOB 2.2 units. Meal eaten 3.5 hours ago (moderate GI).
Predicted fall from ISF (2.0 per unit) and IOB = 4.4 therefore predicted final sensor glucose = 2.5 (hypo)
Apply temporary basal of zero for 60 mins (equivalent to around 0.9 U depending on basal program and time of day)
This should reduce effective IOB to 1.3 units (2.2 minus 0.9) so I should end up around 4.3. No glucose needed.
It is advised that you eat within 45 minutes of completing your exercise. Waiting longer than 45 minutes will greatly increase the amount of time it takes.
Simple sugars will work best. The longer you wait after exercise, the longer it can take. So if you want to exercise significantly everyday, you need to restore quickly enough so that it is available for the next day.
Simple sugars and liquids are fastest, so things like chocolate milk work well.
The problem is, if your BG is high during that time, it doesn’t do anything for you, you just end up peeing the carbs away. So you need to take insulin and carbs immediately after finishing exercise. Sometimes I take the insulin before finishing, just to make sure I can carb-up when I am finished.
The Academy of Nutrition and Dietetics (AND) has a recommendation that active adults and athletes consume 0.5 to 0.7 gram of carbohydrates per pound of body weight post-exercise.
I’m a fan of Skittles. They are 1g of carbohyddrate each (sucrose) so I can pop one or two when trending less that 75 and that’s often all I need to level out. Calories are negligible and they work quickly. I tend to keep them in my mouth as long as possible before swallowing. Here is a link to a study done comparing glucose and sucrose to treat hypoglycemia in Type 1 kids. The effectiveness of glucose, sucrose, and fructose in treating hypoglycemia in children with type 1 diabetes - PubMed
Glucose (dextrose) is the best treatment for lows as it is taken up directly by your cells. Unfortunately many people treat with sucrose (table sugar) (which is 50/50 glucose/fructose) or with things that contain significant amounts of fructose. Just because something is sweet doesn’t mean it will raise your blood sugar. Fructose become such a big component of our diet because it was argued that it was better for those with diabetes because it didn’t raise our blood sugar as much.
So fructose contributes almost nothing toward raising your blood sugar and is directled mostly to replenishing liver glycogen and to production of triglycerides which are deposited as body fat. You deplete your liver glycogen primarily through counterregulation when you have a harsh low.
In my opinion you should try to use either glucose tabs (which are 100% glucose) or candies like Smarties or SweetTarts.
All great information you’ve received here. I too have struggled with weight since diagnosed as Type 1 in my 20’s. With the help of my OmniPod, Dexcom, and very low carb/ low calorie, I managed to lose over 50 pounds and am working now to maintain using the same strategies.
I agree totally with the use of temp basals as a powerful tool. Eating very low carb keeps my numbers fairly flat and allowed me to decrease my insulin needs. I also am one that will usually bottoms out around 60-65 at a really slow drift so I will just run a temp basal for a period of time to allow my numbers to bump up a bit and don’t treat at all in this situation, keeping an eye on my trusty Dex.
When I do have a need to treat an immediate low, I use Coke. Trial and error has shown me that one tiny sip of a Coke will bump my glucose up by 10 points so I treat accordingly and always have a small resealable bottle of Coke with me - purse, office, bedside table. I can treat without overtreating in this manner and limit calories, but these days I rarely need it fortunately. I will also sometimes have a cup of coffee with cream if it’s a slow drift and that provides a slight bump, plus I love my coffee anyway.
It’s taken me years of trial and error to find this level of comfort with tweaks that don’t add calories, but this is what works for me so YDMV. Being postmenopausal now and after 30 years on insulin, I must limit both carbs and calories to control my weight.
I use this same strategy to “use up” unneeded insulin on board that would otherwise require rating carbohydrates. If I’m actually low then I use varying amounts of glucose tablets. But if I can catch a low brewing before it happens, a short0% basal can work really well. I personally find anything beyond 30-60 minutes hard to manage in terms of not overshooting my target and going high. Just today I was 5.8 mmol/L with 0.6 units of insulin on board, did a 30-minute temporary basal of 0% even though I wasn’t dropping, and an hour and a half later I’m 6.4 with a flat line connecting those two points.
I never cease to marvel at how much our physiologies vary from one to another. Coffee, even with the heavy cream that I always use, has essentially no effect whatever on my BG. Yet I know folks who are strongly affected by it. Go figure.
I can’t agree with Eddie enough on this one. Cardio or strength training will deplete stored glycogen, and the muscles can more or less demand physiological priority for refueling. This means they’ll hoover up any available blood glucose after exercise. Combined with exogenous insulin (or even endogenous), this is what leads to persistent lows.
I have found that charting all my exercise, food consumption, and blood glucose levels before, during, and after exercise has helped immensely in understanding how I respond. I’ve gotten pretty good at tailoring my carb consumption to my exercise so that I don’t go low (or high) during or after. But it took months of charting to figure out what my body was doing, when, and how. It took a lot of reading to figure out the why.
Aside comment: It was always a mystery to me how immune I was to lots of strong coffee. Then I did a 23 & Me evaluation and, sure enough, a lack of sensitivity to caffeine lit up. No blood glucose response for me either.
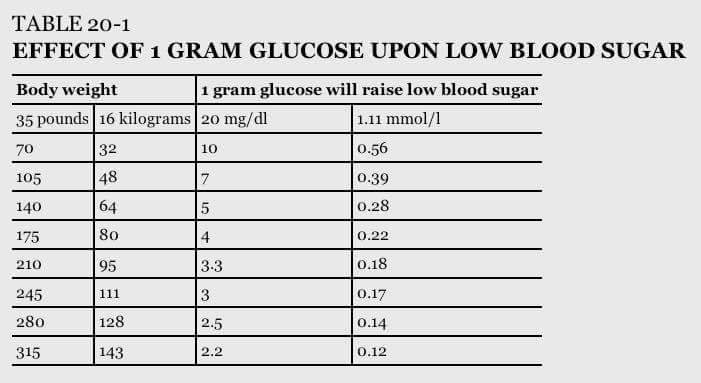
I also use glucose for lows which are at least 60 or below. I use part of one tablet, jelly beans, smartees, or sweettarts for lows that just need a little nudge and dinner is very soon. In that case I take just enough to bring me to target, and then go ahead and eat. Halfway through eating the meal, I bolus as I forego prebolusing in this instance. I also eat the carbs first, but remember I had a fast acting nudge earlier before beginning the meal. If a low happens nowhere near mealtime, I follow up once in target range with usually a spoonful of peanut butter to keep my bg stable. I think it is really important to know how much 1 fast acting carb will raise your bg so as to not overtreat. This is different for everyone. Also know that a fast acting sugar is not going to stick around and will bring you up and then you will go back down, hence the peanut butter.
Congratulations on the weight loss. That took some will power and a bunch of work. Good for you.
@Jen. We seem to have essentially identical approaches. I have never thought of it as “using up excess bolus”, but it’s the same idea. I agree that more than 60 mins at a TB of 0% can cause a jump later.
IIRC you are also a Vibe user. If you set the TB at 0% you get a message that the minimum insulin delivery is 0.025 u/hr. I have assumed this means that you cannot actually set a zero basal, so usually set mine at -90%.