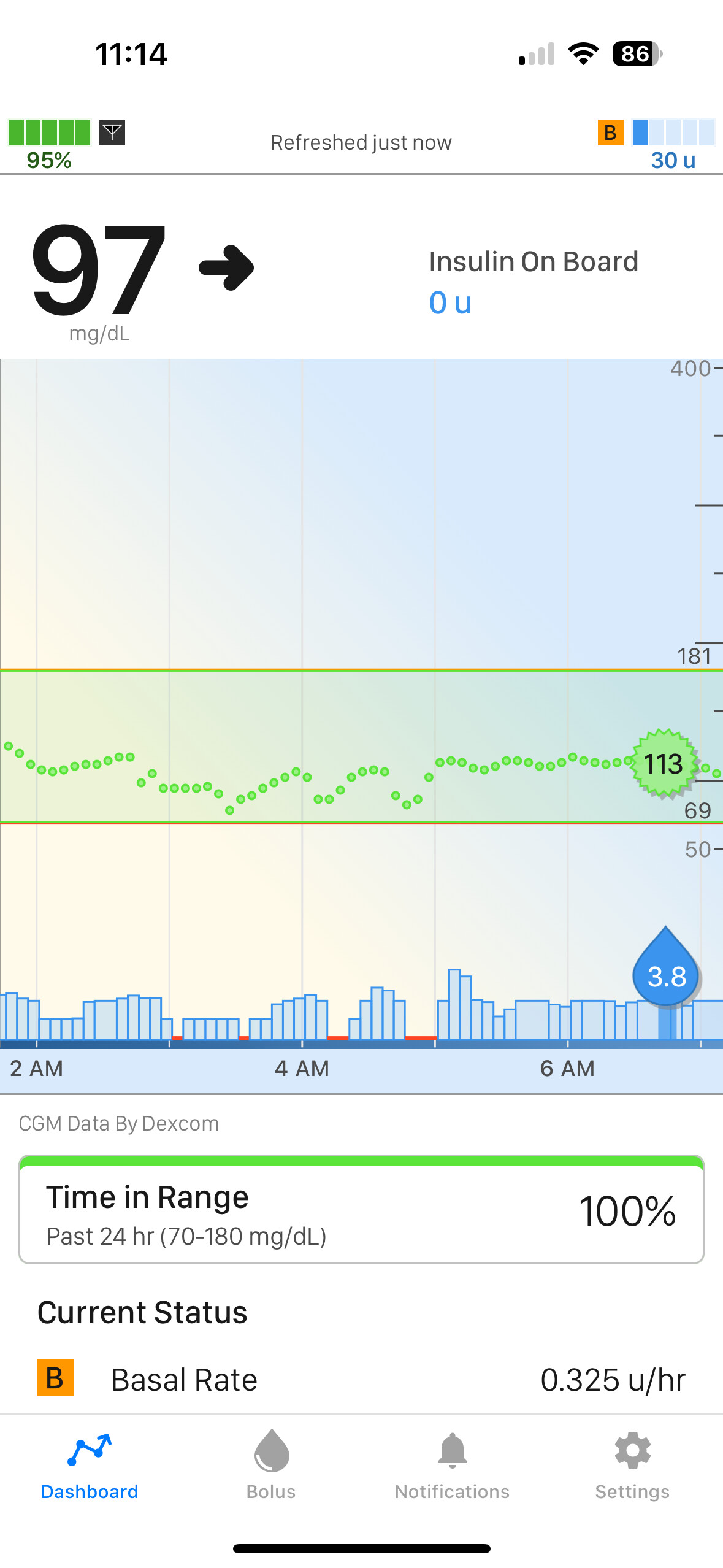
If you post a T:connect screenshot so we can see how the algorithm is behaving and what the various settings are doing, we can explain better. The pump screen doesn’t have enough info. That doesn’t show us anything about Control-IQ behavior in the previous hours.
There are 2 pieces of info you need to understand before we can talk settings and what they do: One, insulin lasts a LONG time in the body. Any individual dose of insulin has potential to lower BG for more than 5 hours to come. It is most powerful/noticable in the first 3ish hours, though, and then continues to work more quietly in the background as it fades away. But this slow activity means you need to look at what happened in the 2 or 3 hours BEFORE any issue arose. Secondly, Control-IQ works on the basis of “net IOB”. Basal insulin is supposed to match the sugar our livers crank out to fuel our constant energy needs. It’s constant. That never really stops. (At least not for T1s without beta cells.) So that basal insulin is null and void. Control-IQ ignores that and only really accounts for insulin that varies from the programmed basal rate. Any insulin delivered that is in EXCESS of the programmed basal rate will be displayed as IOB. IOB is all about how much potential the insulin in her body has to lower BG over the coming hours. IOB may also be negative, in the case of insulin suspension and basal reductions, but we don’t see that. IOB will just read “0” when it’s negative… But new boluses will seemingly disappear faster, because it had to cover the basal deficit. Every adjustment Control-IQ makes is to balance out that net IOB with where her BG is predicted to be in 30 minutes.
To answer your questions about what the settings do:
Basal settings are the very foundation of Control-IQ. That’s the framework the automation is built upon. Setting up good basal rates is step one. This is why testing basal rates is so strongly encouraged. It’s the very first piece of the puzzle.
In the loosest and most general explanation I can offer, with a basal rate that is too high, a person will trend low, or at least below target, and Control-IQ will frequently reduce/suspend insulin to get them back up to target. (It is not the ONLY reason you might have too much insulin on board, though!) It also screws with the IOB displayed, because there is actually more insulin available to lower BG than the pump knows about. This means there will always be a little bit of extra insulin added to adjustments/corrections. Conversely, if a basal rate is programmed too low, that person will struggle with being above target and Control-IQ will constantly be fighting to bring them down. And there is actually less IOB available to lower blood glucose than the pump knows about, because some of that is actually needed to cover the inadequate basal. It’s not really that simple, though. The other settings can mask/complicate things, which is why we start with fasting basal tests and adjust the other settings after. You don’t have to starve her, either. You can break it up into a bunch of mini-tests that are much easier to handle. I actually do believe a good Endo can recognize the patterns, though, and make appropriate adjustments without the fasting, but it’s a slower process. It’s the difference between months of minor tweaking, trial and error, and getting basal rates locked down in a few days with the fasting tests.
Once basal rates are established, i:carb ratio is one of the simpler things to check. This setting is not used by Control-IQ at all. It is only used by the bolus calculator to figure out meal time doses. If she shoots up after a meal and doesn’t come back down, the i:carb setting is too high. If she plummets like a rock, the number is too low. If her blood sugar looks a bit like a rollercoaster where she winds up pretty much near where she was before the meal 3ish hours later, then you found the sweet spot. At that point you may even be able to figure out insulin timing (how long to pre-bolus and does this meal require an extended bolus) to better match food absorption. That last bit is a skill that comes with experience.
And then you didn’t even mention Correction Factor. This is the setting that Control-IQ is using CONSTANTLY to make insulin adjustments and corrections. It’s a biggie. Like, real big. It’s the aggressiveness dial. It sounds to me like the doctor made good adjustments based on the aforementioned patterns, but now the CF setting is causing problems. Because he set up the pump to make more insulin available to the pump with other settings, there might be TOO MUCH insulin available for corrections now. The equation isn’t balanced.
You know how blood sugars are constant rollercoaster of ups and downs? This is the setting that determines if you’re playing on a boring kiddie coaster, a family-friendly ride, or a dangerous extreme thrill ride with giant peaks and plunges. Whenever people talk about the bad rollercoaster, you’ve got to look at that CF setting. A CF that is TOO LOW (smaller number here = more aggressive) means Control-IQ will dose too much insulin when she’s high, driving her low. And do the same exact thing when she’s low, withholding too much insulin and driving her high again. And then the rollercoaster repeats…
On the other side of the equation, a CF that’s too high will essentially cripple Control-IQ. That takes away any power to influence BG. She’ll be high and Control-IQ’s hands are tied. It just can’t help. The CF setting won’t allow it to give anymore insulin. Same with lows. If she’s predicted to go low, it will THINK it’s withholding enough insulin to prevent it, but it really can’t. She’ll just keep trending down until she’s low enough to trigger the full suspend. (Full suspensions are 100% based on Dexcom predictions, and pump settings don’t mean squat at that point)
So the real questions are: Have you done basal testing? Did the meal and inappropriate bolus make her high/low, or did Control-IQ do that?
Also, you’ve gotta ask, are you exacerbating anything by being impatient? Not a judgement here, I’m totally guilty of this myself! It’s hard to sit there and do nothing when this all moves so slow. If you feed a low, you’re double-correcting on top of the insulin Control-IQ already withheld, and you should expect a wicked rebound high. That’s a behavior issue, not a pump setting issue. Control-IQ will actually tell you to eat carbs if it thinks it can’t handle the low. “Control-IQ has predicted that will drop below 70 mg/dl in the next 15 minutes. Eat carbs and test your BG.” And if you do need to treat with carbs, she really needs way less than she would have before Control-IQ. Common recommendations are 5g instead of 15. But of course, that’s subjective.
I’m guilty of comfort eating carbs if I’m low, because it’s the only thing in my power to fix that horrendous feeling. It’s a self-soothing thing, not a medically-necessary thing, if that makes sense. I wind up having to bolus for those carbs just like any other snack!