Caleb’s been pumping Apidra since 2010. Prior to that he used Novolog.
When we started Apidra, I was in heaven. It’s been a great relationship for these many years. However, for several months, we’ve been trying to combat inconsistent highs after 48 hours on a Pod. I was worried he wasn’t rotating his sites enough, so we switched things up - that wasn’t it. We were able to count out whatever he was eating, or growth and say indeed that it appears that the insulin is just not getting in sometimes after 48 hours on a Pod.
We could, and have in the past, just changed the Pod every two days. Apidra made that much of a difference. The issue went away when the smaller Pods came out. But it’s been so many years since using Novolog and changing a Pod every two days is a bit of a bummer, it seemed like it was worth reassessing it’s efficacy.
So on Saturday, we bit the bullet and Caleb filled a Pod with Novolog. What I remember hating most about Novolog is the tail of insulin that would never end. So if we overbolused, it seemed to take great effort to correct. Apidra seemed much more kind in that regard. Also the need to pre bolus was much more of a need on novolog. Not so much on Apidra.
But Caleb is older and bigger and perhaps not quite as sensitive to the difference of these two insulins. I remember asking users - some hailing Apidra as an amazing difference, others (mostly, if not all adults) saying there was no marked difference.
It’s been an annoying start - I don’t enjoy baselining this kind of stuff. I feel like we’ve been there done that and I know it’s something we always need to reassess but, pooey, having to simplify eating habits and schedules seems to pour salt on the wound for someone who has this constant consideration throughout the day. But we’re doing it.
He’s still on the same Pod of novolog and passed the 48 hour mark earlier today and is struggling to keep his bg above 70. i’m curious to see how this all plays out…
You’re smart for switching things up. I know it’s a pain to alter the routine but I think diabetes demands changing treatment sometimes. Holding on to what you’ve always done just because you’ve always done it is not a smart tactic.
By the way, I use Apidra in my pump, too. The Apidra insulin package insert directs changing infusion sets and reservoirs every 48 hours. I usually went to 72 hours without trouble.
Now I’m using an old Medtronic pump with a 300 unit reservoir. I decided to test the viability of Apidra for a longer time in the reservoir/infusion set. The Apidra now stores in the resrvoir/infusion set for nine days.
I am on my third set doing this and no trouble. Maybe I’m tempting fate, but I like this new routine of changing my reservoir and infusion tubing every nine days and changing the infusion site every three days. It seems to be working well.
Interesting. When Caleb started Apidra, we used vials, but then went to pens simply bc it was less insulin out of the fridge at a time and less likely to go bad. I’ve really never found leaving the insulin out to be a problem though. This approach was precautionary. I often don’t refrigerate on vacation bc the risk of forgetting the insulin in the fridge or the fridge freezing is worse. And yes, we have a frio pack, but I find that only necessary when we are out in the heat for the day.
So I’m not surprised that it keeps in your reservoir. I really don’t understand why we are having this problem with Pod. It came out of the blue after no issue for years. I got a whole new batch of insulin and still the same issue. The insulin drips out of the cannula sometimes when he takes off the Pod, which implies it comes out of the cannula freely, so it must be a Caleb problem, but it doesn’t matter where we put it on him, so it’s not a scar tissue issue.
This conversation came very useful. I’ve been on a insulin pump for more than 10 years now, always used Novolog but tried this month Apidra just because of the cost (it is cheaper in my country). I had read and knew that perhaps a change of set and reservoir would be needed. I am absolutely positive I am using novolog again (since the reservoirs and quick sets are a lot more expensive here than an insulin vial). I could use novolog in the same reservoir for up to 5 days without unexplained high bg’s. Good to know you have been lucky, perhaps I´m missing something.
I stared on Apridra when I was on MDIs. I didn’t want a pump and we were trying everything we could to get me to my A1C goal. Apidra got me the closest to that goal but it took agreeing to try a pump to get me to the “magic number”. Anyway, I pumped Apridra for about 8 years until my insurance company forced me to switch a year ago. I fought and was denied. I was sure Novolog was going to be a train wreck. But it worked just fine from the start, and I think it may even work better for me. I feel like I don’t have as many severe lows as I had on Apidra, and that isn’t coming at the expense of more highs. My A1C has held steady over the year with Novolog and I feel very lucky that it worked out so well. I hope it works just as well for Caleb!!
It’s not a “Caleb problem”! I have noticed the same thing on occasion, the pod will just go south on me after 2 days. I have heard that the ADA actually has studies for this, and there are expectations that for each successive day of wearing a pump (not just omnipod, but any type), people can anticipate a certain degree of higher BG. I think it’s crazy that they would just say that without making a recommendation, such as increasing bolus and basal amounts…
If you think what it would be like to inject with a pen or syringe in the same exact spot for 3 days - how someone’s body might respond to that. I guess it is not terribly surprising that 3 days in the same spot with a pump makes things flaky.
Perhaps a once-a-day shot of lantus or tresiba would help, because it would reduce the total volume of insulin being delivered in that infusion site. If you give 50% of his total basal needs with an injection, you could then use the basal adjustment on the PDM to adjust the remainder up or down. The only difference is that instead of being able to adjust basal from 0-100%, you could only adjust if from 50-100%, because you have 50% already locked in with lantus or tresiba. Just a thought. Let me know if this needs clarification…
I have never had insurance coverage for Apidra and thus have never tried too hard to find it better than Novolog. I am always amazed at the people on TuDiabetes who seem to effortlessly get coverage for Apidra, Afrezza, Tresiba, Toujeo, and all of the new stuff. That is not my insurance world. But I manage fine with a pump filled with Novolog and would have a difficult time persuading anyone that I need anything better. But I sure would like a super fast insulin…
I have posted on this before but to recap, of the three rapid acting analog insulins, Apidra is by far the most prone to site degradation issues. This is evidence-based. I won’t go into the details but I switched from Apidra to Humalog because I was struggling to get my sites to last even 48 hours and found it a big improvement. Novorapid (aka Novolog) is the least prone to site problems but as the OP points out, can have a longer tail than Apidra.
Novo’s new rapid acting analog insulin Fiasp has just been approved in at least one EU country. I am waiting for it to be added to the “approved” list in the UK and will give it a go. Apparently the plan is for it to replace Novorapid entirely.
Maybe not, but I really think it’s specific to Apidra and not just any insulin. Our first Pod of Novolog has gone the whole 72 hours and could probably make the 80 but Caleb will be in school so he’s changing it now. He’s 76 downward arrow, so insulin is still delivering. It’s a significant difference to what we’ve been struggling with. However, we can’t draw a conclusion from just one Pod!
Day one on Novolog was a nightmare. Day 2 better and Day 3 a dream. Here is is overnight, which was after a correction - no crazy tail of insulin to contend with. The correction was needed bc I asked him not bolus for dessert bc he was low before bed the night before. My fingers are crossed this type of result is not a fluke.
I remember reading the reasoning behind this when we first noticed this issue years ago - I remember it as bc it breaks down faster to activate, it’s more prone to simple breaking down. Haha - so over simplistic and non clinical and perhaps not even accurate, but it was my interpretation.
Just wanted to share this. Apologies if you have already read this. And a quick disclaimer, I have never used Apidra in a pump, I have only used it with injection.
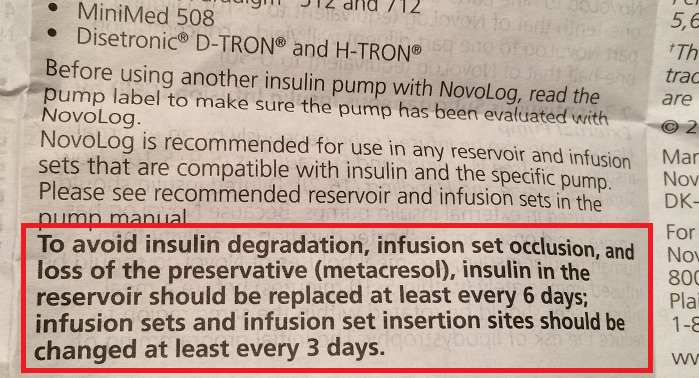
One of the things that struck me as very strange was how the inserts for both Humalog and NovoLog said 3 days for infusion site, and 6-7 days for the reservoir. But Apidra said 2 days for the reservoir! And for Apidra, I didn’t see a mention specifically for infusion like I did for the other two.
Jaime has been using Apidra and Omnipod; we love how Apidra works. We do get a couple of pods a month were the bg goes a bit higher especially that 3rd day. But, even though we see insulin dripping from the cannula seems to be bent. So we have been assuming that due to the lack of fatty tissues the cannula has been hitting muscle.
Whenever that happens, do you correct the bg with a syringe? How does the Apidra behave? That’s how we have learned, for us it’s not an insulin issue, it’s a bent cannula.
A major contributor to site degradation is the denaturation of insulin around the site and in the cannula. The denatured insulin forms insoluble fibrils that can cause blockages or reduced absorption from the tissues at the site. Denaturation can be caused as a result of carbon dioxide in the tissues locally reducing the pH (i.e. making them more acid). Because each of the three analogs use different amino acid modifications to achieve rapid uptake, the three versions of insulin have different stabilities at reduced pH - Apidra being the most unstable.
As there is no CO2 in the reservoir, this shouldn’t be affected.
Caleb never has bent cannulas - not since using the smaller Pods. We’ve testing this issue with Apidra before and it’s very familiar how the Novolog acts differently than the Apidra. We’ve been assessing this recent occurrence since September. What leads me to conclude it’s the insulin is that elephant doses of corrections via pump do little, then a new site and voila - it’s fixed. So, no, not a syringe correction, but similar.
Personally, I do. If we get through another two full Pods without and second/third day highs, I’ll feel very confident, although I’m pretty much already there. It’s a matter of deciding is Novolog’s tail can be tolerated, and if not, then it will be 2 day Pod changes as a rule w Apidra.
Any thoughts of doing this? If you reduce the total volume of insulin, could that make a difference?
For example, if total basal is 20 units per day, and you take out half of that amount with Tresiba, you’d reduce the total amount infused at the site by 30 units over the course of 3 days.