This is happening quite often lately.Today I was 90 before lunch, then 60 grams of carbs (white rice and fruit; papaya and banana) and 6 units of apidra (injected), some fish and lots of salad. Then 2 hours later I was at 141. And 35 minutes after that (just sitting in my office, no special high level of activity) I was at 70.
Like I said this tends to happen quite a bit lately. 2 hours after eating I might be in good range and then a super fast drop (70 - 90 points) before the next hour. It's specially hard at night, I usually have to set the timer 1 hour after going to sleep to eat something and not go low during the night.
This sounds like classic reactive hypoglycemia. If you are still making some natural insulin your body, when you eat it may cause a surge of your own insulin to cause you to go low 2-3 hours after eating. If this is the case you may find some relief by reducing the amount of carbs in your meals.
I have no experience with reactive hypoglycemia, but think that is unlikely if you're a T1.
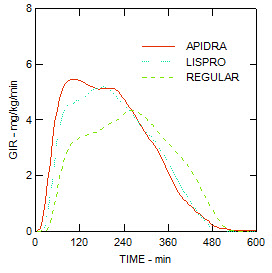
To me it sounds like you are simply experiencing the effects of your insulin bolus. None of the fast acting insulins (Humalog, Novolog, Apridra) disappear after two hours. Apridra is still somewhat active after two hours - and if your food is all digested it can cause your BG to go down. Check out the action graph at the bottom of the page.
You could try taking a bit less insulin and eating your carb at the end of your meal instead of the beginning, or saving some of the carb as a snack for a couple hours later, etc. Now that you've identified the issue you can adjust things until you make it work. Also, it is not a good idea to go to bed just a couple hours after eating - try eating earlier (or maybe staying up later :) to get your BG/active insulin taken care of before you go to sleep. I naturally eat late at night, but changing to be sure I had my BG resolved before going to bed has made a big improvement for my BG predictability.
I do not have an answer but just wonder about fish meals. For me, a pump user, when I eat a fish entree, I have to remember to use less insulin bolus than with any other entree. I also eat at least 60 or more carbs in some type of bread, plus salad and a vegetable. You may live where you eat a lot of fish and this may not be your issue. And I have no explanation as to why I can eat a big fish dinner and need less insulin but it is true. Whether fish is baked or fried. As a long time T1D, I have no natural insulin!
While the action of fast-acting starts in kinda the half hour timeframe, there is still a lot of insulin activity actually continuing in the 2-4 hour region so we shouldn't be surprised at hypos at that time.
But like you, I am sometimes (rudely) surprised at post-meal hypos!!! It is very disoncerting to have post-meal hypos, really throws me for a loop. Almost makes we want to have the Monty Python guys come in and declare "Nobody expects the post meal hypo!"
It is not uncommon for someone with T1/LADA to have their insulin production come and go a bit in the first years after diagnosis. That may be what is happening for Santiago.
You should talk with your doctor. if you are going low one hour after sleeping you maybe using to much insulin. Sleep is just as important as glucose control and while that sometimes runs counter the messages we get, I am betting if your doctor knew you were eating one hour after sleeping he/she would adjust the dose at some point. I would not try to do that without discussing it with a doctor or CDE however. You have way to many variables going on to go this alone. Get an expert, doctor or CDE, involved.
Thanks for your insightful comments everyone, I guess I'll just eat something 2 hours after injecting, who knows what's going on, but the important thing is to keep BG balanced.
That situation was pretty common for me while on MDI, except it was not reactive hypoglycemia, it would happen at what appeared to be random times throughout the day.
I would be happily going along at 140-150 then within minutes (sometimes as little as five) I would drop up to 80-100 points! The month before going on the pump I think I had something like 45 or so moderate-severe lows (a couple in the 30s). All of this was happening while my doctor & I continued to reduce my dosage. In a six week period, I reduced my TDD by 35-40% and was still having this effect.
Prior to that six-week period, my BGs were steady as a rock. I could count the number of lows for a full year on one hand!
Been on the pump for about a month now and only had once such occurrence and only two lows total! Which confirmed our suspicion that it was inconsistent absorption of the intermediate-acting insulin combined with a marked increase in insulin sensitivity and/or a reduction in carbohydrate intolerance.
TDD now, on the pump, is less than half what it was before the pump.
And just to complicate things even more, I have noticed that, for me at least, there is not a linear relationship between Carb intake and insulin requirement. If I eat when my BG is in a certain range, my insulin requirement is significantly lower (sometimes by half) than if I eat the exact same meal when my BG is in a higher range.
For example, if my BG is, say, 90 before I eat I need 6 units; but if I have the same meal when my BG is 120 I might need 12-13. That is far more than what one would expect when the correction factor is added in (to reduce the 120 down to my target of 110.)
this happens to me too, probably all of us at some point. your basal may be too high or maybe you're digesting a food more quickly. or it could be some activity you did a few hours earlier...kinda sucks because there are so many variables. maybe cut back on your I:CR, prebolus if you're not. good luck!
This sometimes happens to me too usually with activity after the meal(low after meal) too depending on activity before and after the meal, bg before the meal and other unknown factors. What I do is have a snack if I feel like I'm dropping and always reduce my bolus dose and sometimes skip pre-bolus depending on all the factors. I usually have most of my carbs at the end of the meal for dinner with yogurt/berries but you could try adding in a carby treat at the end or after the meal if reducing bolus doesn't help at all. I hope you get this figured out. I think there are so many factors we can't really determine like absorption rates on a particular day and activity effects and varying absorption of insulin.
i was thinkin prebolus to not get the spike, if that's happening, then the drop. trying to match the insulin with the carbs. easier said then done. Not sure if the OP wears a CGM, as one can really see what's happening right after a meal, the spike and then drop.
Yeah, prebolus can be variable for me because sometimes I drop like a stone and go hypo during the meal and other times I spike like crazy if I don't prebolus. cgm if accurate would be great because you would have some idea of what is happening. Maybe he can try that to see what is happening with him, or he can test through the meal and after and see what is going on.
The data sure looks to me like two things together: Incorrect I:C, and not pre-bolusing early enough.
Do some experimentation to really nail down your I:C. You have to account for the tail of the insulin, so give yourself 4 hours before you conclude that you no longer have any IOB. Any carbs you end up eating to head off a low should be added to what you ate for the meal.
Then, with a more accurate I:C, start experimenting with bolusing early to determine how far in advance you need to adminster insulin to better control the spike.
I get a similar profile if I take too much insulin, and take it when I eat, rather then 30-40 minutes before.