That’s an interesting approach, and I hope you have success with it @Jen. Infusion set failures are very frustrating even when they happen infrequently, and I can only imagine what you are dealing with these days. Best luck! Regarding allergies, a side question: have you had your vitamin D level tested?
No Vitamin D level checked. Though I’m sure between autoimmune diseases and many allergies (both associated with low Vitamin D, I believe) and living in Canada, my Vitamin D level is probably low. When I asked my GP about it he brushed it off. It’s a test I’d have to pay for even if I did get my GP to order it, and I’m not sure how much it costs. Might see if he’ll reconsider next time I have an appointment. I’ve had both allergies and diabetes since I was young, though, so neither one is new and I’m not sure how much Vitamin D would change the course of things.
I used to have some mild skin rashes under watch wristband, as well as around infusion set sites. About 5 years ago I had Vitamin D blood test ordered by my endo, and it was found to be very low. She told me Vitamin D deficiency is very common among people with T1D. She prescribed some large supplement over couple of weeks, followed by over-the-counter daily dose. I have since been taking 4,000 IU daily, my level is in what is considered normal range, and I no longer have any skin rashes. There is a lengthy discussion about Vitamin D at Linus Pauling Institute. I would not expect any miracles, but it would not hurt to check and, if need be, bring Vitamin D to a normal level.
1 Like
I think your advice about Vitamin D is probably good for all of us, thanks.
I have truly enjoyed reading (and felt a kinship with the posters) As most of you know I have had many probnlems with my current Endo practice because I strive to noj-D numbers (and usually am pretty successful - but all have our ups and downs). I have had to show CGM printouts to prove that my A1C isn’t an average of extreme highs offset by extreme lows. (I really want to ask if this practice thinks that upon Dx of D you also should be Dx’d with the co-morbidities of stupid and lazy - they have such a low opinion of their patients. At least that is my experience). ANyway, I like to describe myself as approaching my D the same way I approached coloring books - I like to stay within the lines.
I allow myself a range - a range that is close to what people woithout D experience. And most importantly, what I do works for me - and I believe I have a say in my treatment since I am the one who has to think like a pancreas (that’s Gary S for that phrase)
1 Like
I whole-heartedly agree with your approach on this, @artwoman. Unfortunately the coloring books that PWD use do not match up with the coloring books of the docs. If I use the docs’ coloring books, I clearly draw outside of their lines and I righteously do so. They don’t have to live in our bodies 24/7. They don’t have to live with the complications that arise from years of following their “permissive hyperglycemia” tactics. I only have my body to look after. I agree with you, as close to normal BGs as possible, thank-you very much!
Remember for every patient like you, your clinician probably see a 100 that don’t invest the time, energy, and attention that you do. I think the docs have been beaten down by the aggregate effect of their patients that don’t want to be inconvenienced too much with their condition. It would be hard seeing 3, 4, 5 patients an hour every day and witness most patients’ A1c’s north of 7% or 8% or more. They talk to most patients that don’t want more test strips to use, but want to test less.
When the docs finally see someone like us they tend to not believe their senses and instead doubt that we are the real deal. They’re seen so much variability and outright BG rollercoasters they don’t think that an A1c of less than 6.5% can be had without excessive hypoglycemia.
I used to be angry with docs because they don’t get people like me. That’s OK. They have a tough job and the system in the US just beats them down and wears them out. Count me in as a member of the “smile and nod” club. Just give me my scrips and watch my blood tests and I’m OK with that. But don’t try to give me any advice on dosing insulin! They have no idea about the game I play.
You are far more forgiving than I. My former Endo - who like so many other MD’s no doubt had patients who didn’t(or couldn’t) make the efoort. In turn he greeted me with hugs, appreciated that I proved that at least for me (Zoe is correct different folks have different needs/approaches/etc). His taking pleasure in my successes, only served to motivate me even more.
Currently, I am accused of lying about my bg’s, given handouts that to qualify for a pump I have to have uncontrolled diabetes (I’ve been pumping for about 12 years now - long before I met them here - and I ask if maybe my control is due in large part to my being a pumper (and my willingness to pay out of pocket for my Dexcom). Part of my challenge right now is that I am living in a new city, and still trying to find an Endo who accepts my tight mgt, and then find which health plan network they are in.
As to coloring books, I always embellished the images in the books, gave the pictures fancier clothes, more stuff in the scenery etc. i.e. I ,make my own lines in the coloring book.
So terry4, what city do you live in, can you give me the name of your good Endo?
1 Like
I live in San Francisco. Don’t you live in Portland, Oregon? I will be moving there next March. I’ll be looking for a new endo as well. Or I might commute to San Francisco to stay with my current doctor. I intend to take up a full-time RV lifestyle and I thought I might get set up with a doctor at the Mayo Clinic in Phoenix. I went there for another reason a few years ago and I love the way they treat patients.
My current endo is a woman who I like because she communicates well. I still think she doesn’t fully appreciate what I do. I thought for a time that she might have some professional curiosity about how I get the results I do, but no. That’s where I think the clinician’s schedule demands are a grind.
Not a flatliner so to speak, but I’m starting hour 37 of a no hitter! High alarm is set at 150, low at 65!
5 Likes
Excellent! I’d call that flat-enough! Great work - keep it going!
2 Likes
I’d call that a flatline, too! What caused this bit flatlining? An early New Year’s Resolution? Or just the recent full moon??! Good for you @MissMargie!
Not quite a flatline, but the best 24 hour period I’ve had in a long time.
I had a 35g low-GI breakfast (steel cut oats, almond milk, pumpkin seeds, almonds, and berries), and took 20% less bolus insulin on a hunch. During the morning I tried to prevent a low by eating 20g of fast-acting carbohydrates (two small cookies), but I still went a little low before coming up.
For lunch I had 24g of low-GI food (almond yogurt, berries, and a small piece of chocolate). However, I was heading in to a 2.5 hour teaching session where I find it very difficult to glance at my CGM (since I have to bring it up to my face to see it, so it’s impossible to do discreetly), and since I’d had a low during the morning I lowered my I:C ratio and also lowered my basal rate by 0.1 u/hr. But then I made a mistake—I decided to eat a 10g cookie “just in case” I went low. Instead, I went too high. What’s interesting is that even though I corrected with a unit as soon as my high alert went off, my BG continued to rise quite a bit for the next hour until the insulin finally kicked in—definitely a good illustration of the lag time of insulin. (That tiny “mistake” led to two hours out of range, but it could have just as easily prevented a low…) Then, when it did kick in, it lowered my blood sugar a bit too much, so I ended up having to eat about 13g of fast-acting carbohydrates on the way home.
For dinner I had 20g of carbs of low-GI food (butternut squash soup and chicken), but perhaps I’ve under-bolused for it as my high alert just went off (perhaps I was wrong in reducing my I:C ratio at lunch…). Or, maybe I didn’t pre-bolus far enough in advance, which I find challenging to do on work days (I’m either rushing out to work in the morning, rushing between meetings and off-site appointments during the day, or arriving home starving).
2 Likes
Nice BG day, Jen. Your pre-emptive cookie could have gone the other way. D is so capricious. Do I act on my first approximation of my expectations, or the second, or the third …
Very good 24-hour period @Jen, and very nicely explained! I tend to make exactly the same ‘mistake’ of taking some extra carbs ‘just in case’ before work situations when I know I would not be able to easily make carb corrections.
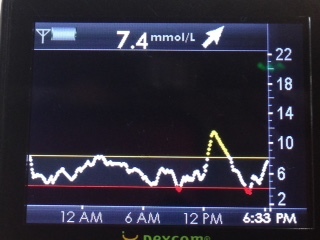
Ok, After a VERY rocky holiday weekend (which started Wednesday and went thru Saturday), I managed a pretty solid landing:

That continued … until I took a chance at gasp LEFTOVERS tonight for dinner:

… at least I think I landed safely.

2 Likes
That’s a sweet line, @Thas. Even the left-over bump is short-lived and quickly returns to in-range BGs. Good work!
I am calling that a “no harm, no foul” spike! Nice recovery!
The past few days I’ve been spraying Flovent on my sites before inserting the infusion set. I’m not sure if this is safe long-term, but someone else with Type 1 suggested it, I read about it online, and I happen to have Flovent on hand for other conditions, so I decided to try it. So far, so good—I’ve left both infusion sets in the full two days with neither one getting irritated or randomly dying.
So, I feel like I’m back on track (at least for now…I’ll have to discuss using Flovent with my endocrinologist).
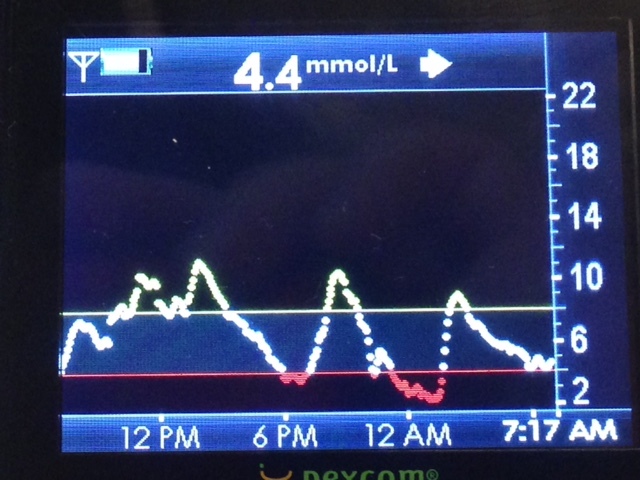
Yesterday was a bit crazier than the day before, despite eating similar food in terms of carbohydrates. The day before I spiked high at lunch and dinner after lowing my I:C ratio and basal, so I put my I:C ratio back and left the basal the same. I then went low overnight so I lowered just my overnight basal segment but left the rest the same.
Yesterday after breakfast (45 grams - steel cut oats, almond milk, pumpkin seeds, almonds, apple) I went high and then just never came down. Perhaps partly my own fault for then having a “snack” of 24 grams during the morning. But even after several corrections I was still high.
For lunch I had 24 grams (salad and a bit of chocolate) and during the early afternoon I put my basal rate up by 1.0 units so that it was the same as it had been about 24 hours ago. But then the correction brough my blood sugar down too low, but this was close to dinner and wasn’t very low, so I didn’t treat it.
I spiked after dinner (eggs and toast and almond butter - 40 grams) even with both the basal and I:C ratio back at their highest.
Then, overnight I woke up to my Dexcom screaming “LOW” at me, ate 18 grams of sugar and went back to bed. Woke up briefly to my Dexcom alarming high but did nothing about it, and yet by morning I’d fallen back down to the bottom of my target range. Clearly my basal is way too high, at least overnight…
Today I’m going to try and not have a 24 gram “snack” this morning and see how things go before making any other changes. I’m thinking that I need to lower my basal rate and keep my I:C ratio the same but make sure I pre-bolus longer before meals, which I have not really been doing. It’s by far the most challenging thing to pre-bolus by 30-45+ minutes during the workweek. I really don’t know how the endocrinologist who wrote Sugar Surfing sometimes waits an hour or more before eating without having to dig into breakfast while seeing patients!?
Jen, I think it’s tough to do the troubleshooting you do with the allergic site reactions in the mix. It makes my tactics seem like child’s play! Any way, just want to add encouragement. I hope the flovent thing pans out. That might help you a lot. 
[quote]Jen, I think it’s tough to do the troubleshooting you do with the
allergic site reactions in the mix. It makes my tactics seem like
child’s play! Any way, just want to add encouragement. I hope the
flovent thing pans out. That might help you a lot. [/quote]
I feel like my control for the past few days has been back to “normal” control without any site interference. Here’s hoping I’ve found a solution so that I can get back to seeing 24-hour flatlines!