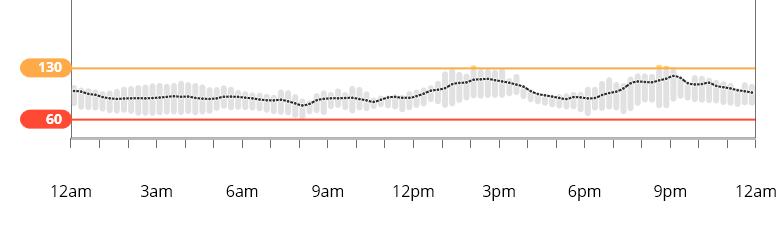
First alarm-free overnight in weeks. I’ve recently had to bump up my overnight basals a lot. Then they were too much and produced hard-driving sustained lows even with abundant glucose tabs. When the basal lows finally turned around they’d bounce high. Persistence paid off.
Very nice overnight @Terry4! I’ve been trying to make some overnight adjustments lately to stop some slow drops I’ve been having - no low the last couple nights, but it took a small handful of mints on the way to bed to accomplish. It’s so difficult sometimes to get those longer stretches right. Good job!
Thanks, @Thas. We know good control is a moving target but sometimes our surfing efforts include a few wipeouts!
I finally learned that the best way to treat a too-agressive basal low is to, in addition to treatment carbs, turn off basal for 30 minutes. Some of these lows lasted 90 minutes, even in the face of 15-minute additions of glucose tabs. I tried not to overdo the glucose tabs and only took one or two every 15-30 minutes. The 30-minute basal turn off, at first alarm, was key.
Ok - you made me dig out my numbers Here’s what I had one night last week:
The first attempted rise was a feeble attempt (apparently) to fix the low. The second was my liver kicking in some DP “support”… followed by breakfast.
That’s what makes treating lows an art in itself. You want just the right amount of glucose and no more. Did you know that for the average weight adult male, 100 mg/dl = 1.25 glucose tablets?
Yes, your math indeed works out, makes sense. Let’s assume one is in equilibrium with perfectly flat BG line in range, the basal rate is set perfectly, any prior meals have been digested long ago, and the person is not changing the level of physical or mental activity. Then, if that person with T1D would have 1.25 glucose tablet, the BG would still not increase by 100 mg/dl, would it? I understand the majority - an equivalent of about 3/4 of 5 grams - would be stored in the liver in the form of glycogen, while the BG would increase by about 25 mg/dl. Does this sound correct?
I don’t know what percentage of the inbound glucose that the liver would claim. There is also the issue of the amount of glucose the liver may release. I am at the limit of my understanding.
There are just enough variables in the system that it’s hard to reduce all this to an equation. It’s a dynamic system that we don’t necessarily understand or even need to understand all its component pieces. Instead we really need to watch the overall trends and move in counteracting ways to keep things as balanced as possible. Ponder’s surfing metaphor really captures this for me.
Agreed. We do not necessarily need to understand the underlying metabolic pathways, which are complex, highly variable from person to person and from time to time even for the same person, and probably not fully understood even among experts. I was just curious about the discrepancy between what your math would imply (+20 mg/dL per gram of glucose), and what is commonly observed (I’ve seen +5 mg/dL per gram quoted as an average for an adult, which roughly matches my own experience). Liver is a storage unit with input/output modulated by insulin concentration, which is what may provide at least a conceptual explanation.
I read some interesting comments on this topic on the DIYPS website about a year ago. Scott Leibrand and Dana Lewis wrote about using a small early prebolus to get the liver involved earlier in soaking up more glucose after a meal. I forget the exact dose but it was on the order of one unit of insulin or less given about one hour before eating. The early pre-bolus size was based how high above your target your current BG was sitting.
Your explanation about the liver’s role makes sense but it’s quickly complicated by other factors like meals, continuing exercise response, lack of sleep, stress and illness to name just a few. Yes, it’s my understanding that the liver’s ability to store glucose is modulated by the presence and amount of insulin available. I think that’s one of the reasons that insulin delivered in a timely fashion for meal metabolism can be fewer units than required to pull down high BGs later due to a late insulin delivery.
Nice improvement over the travel time. The tight 15-min slices come from a fairly boring eating pattern - not all that much variety these days. But, I think as we’ve discussed before that time-in-range (TIR) is possibly one of the biggest factors to consider. I like that my last 14 days were almost 89% in-range (91+% the last 7 days). Perfection isn’t happening, but I’m aiming to keep TIR up there, as much as I can.
I don’t know if I’d say you need to do better @Terry4 , that “spike” is well within normal results observed in people without diabetes!!
I also don’t vary my diet much. This week, I made a large pot of chili on Sunday and have been eating it alll week. The Fritos only lasted through Monday though…
As an aside, for those that understand that the three sail lines that control the sails on a sailboat are also known as “sheets,” it gives meaning to the expession, " three sheets to the wind."
Please excuse my digression. I am an unreformed sailor.
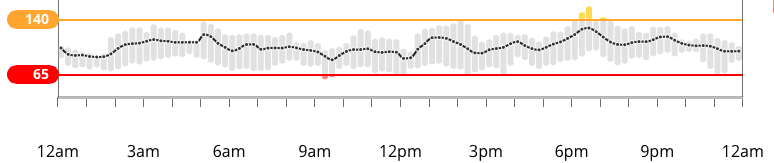
 red line = 65 mg/dl, yellow line = 140 mg/dl
red line = 65 mg/dl, yellow line = 140 mg/dl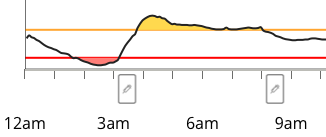
 Here’s what I had one night last week:
Here’s what I had one night last week: