My body has gotten into the bad habit of raising my BG starting at 3am. It has been going on for years. BG can be lowered with insulin, obviously. What are the other ways y’all have found to reduce the BG rise? I’ve found heavy exercise or activity during the previous day helps.
If anyone has found a resource that talks about the biological processes that cause the rise backed by research I’d love to read it. Everything I’ve found boils down to “Yup, sure happens. Look at the liver go.” I’m interested in why it happens.
@spdif My understanding of the dawn phenomenon is that it is a natural part of the flight or fight syndrome that does not cause hyperglycemia in those without diabetes mellitus. The paper I’m going to link to suggests what I think is the cause.
As we near our waking time there is an elevation of human growth hormone and cortisol causing an increase of insulin resistance and stimulating the Alpha cells to secrete glucagon which stimulates the liver to convert stored glycogen into glucose.
In normals the rise of blood glucose is not allowed to rise above 99mg/dl. For us with impaired glucose regulation this is not the case. Dawn phenomenal can be controlled with a correction bolus of insulin, but is a real problem for T2DMs that don’t use insulin. Metformin is helpful because it inhibits the liver glucose dump somewhat and increases insulin sensitivity a bit.
Feet on the floor syndrome may have the same mechanism as the Dawn Phenomena. This is a rise of BG that begins when your feet hit the floor, continuing to rise.
The Somogyi Effect Is different it occurs when BG drops around 2-3 AM and there is an over reaction by the Alpha cells.
When I am on a LCHF diet, I do not get any dawn phenomen, ever. As soon as I add even a little protein to gain muscle mass, dawn phenomen kicks in almost instantly. I do generally eat OMAD (one meal a day) at lunch.
@Luis3 I’m really glad you posted and I’m hoping people with T2D stumble on this like you did. Metformin is absolutely an option if I can’t find a diet/exercise/lifestyle change solution.
@CJ114 When you eat LCHF how many grams of carbs per day is “low”? I’m curious how you sustain a diet with 0 protein. I know I eat more, maybe double, the average daily recommended protein as a way to fill up on anything but carbs. I’ll have to look into if anyone has explored proteins role in DP and experiment with some different foods.
@spdif 20g carbs is daily target. - OMAD consists primarily of avocado or cream cheese lemon cheesecake. I don’t do 0 protein, just do not add any. In other words when I have avocado on some lettuce, I do not add a few slices of ham, or turkey, or shrimp as that would give me DP.
T1D here for 67 years. I’ve discussed this with my Endocrinologist, and she showed me the list of about 47 causes for this. All ya can do is to ask “why me?”
In my 60+ years of T1D I never found a way to prevent it. On a pump I have been able to program a large increase in basal rate. I have tried low carb, difficult to maintain for many years, and no effect. I have tried not eating after dinner- no effect. In the past 2 years I have been also experiencing a high 20 min after going to bed, ranging from an increase of 50-100 mg/dl.
One thing that can affect dawn phenomena is statins; they tend to increase BG. It’s in the patient information.
Is dawn phenomena party of flight or flight? It is the same mechanism, counterregulatory hormones. But I thought it was a natural effect of circadian rhythms, moving to the wake part of the cycle.
And I don’t think rebound (somogyi) is over reaction. IIRC, it IS part of flight or flight. Or at least it behaves in the same way. I could be wrong and invite corrections. After all, I never heard of feet on the floor syndrome in my 50+ years with T1.
As I understand, different counterregulatory hormones are released at different times and bG levels during a hypo. In both cases the body is trying to raise the bG as quickly as possible.
In fight or flight, the threat may not abate even if the immediate danger, or perception of it, has diminished. So the increased glycogenesis can president for up to 24 hours. With a low bG, it is obviously avoiding a severe low, but it also provides energy to hunt to get food.
In any case, you make an excellent point that “dawn phenomena" may actually be a rebound from an overnight low. If so, treating it as a circadian spike in CR hormones, ie more insulin, can make things worse. As a general rule, one should make adjustments to eliminate hypos before adjusting for highs. Don’t adjust for a high if there was a hypo during the previous 24 hours.
For me it took multiple adjustments in my pump settings to get it right. I typically go really low before BGs start to rise in predawn hours. I am attaching my settings just to clarify. Obviously everyone is different.
I know my first reply referred to insulin and you want ways other than insulin to lower predawn BG. I have noticed that my BGs are lower since I increased my daily exercise. Good luck. Let us know what works.
It’s been a while, but I increased my basal insulin to cover most of “feet on floor” syndrome. I also used a very low carb ratio for breakfast and added extra insulin. It only worked because it occured about the same every day. The one catch was, if I ate more carbs than usual too much insulin was calculated.
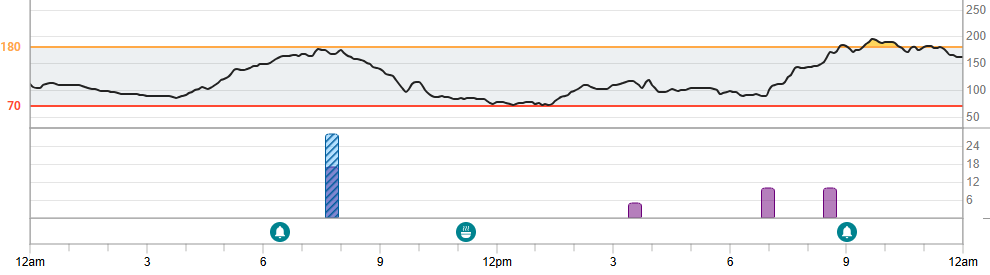
A picture is worth a 1,000 word. @TJG never heard of FOTF syndrome. Last night I had no Dawn Phenomenon BG rise, but a steady rise after I got out of bed. The pump increased basal to its 1.4u/hr setting, but couldn’t stop the rise. So I bolused 1..5u.
Don’t take any of the below as medical advise. The “spikes” can very resistant to treatment and take a long time to come down. I often end up dealing with a hypo episode when BG finally comesdown.
I see you are T2 (assuming you weren’t misdiagnosed). I had a language professor who came down with T2 and was having a problem with BG going high at night. Her and endo’s solution was a small snack before bed and that worked for her. Running low on carbs apparently triggered the liver to dump glucose.
Your added insulin might be mis timed (or insufficient). Absolute minimum time for my insulin to have an afect on BG is 45 minutes. What I had been doing was programming extra basal starting a couple hours ahead of my alarm. So I was cheating on my basal to get ahead of “spike”.
I’ve had a couple of endos tell me that I was using too much insulin and the extra insulin caused insulin resistance. So their solutions was to back off on insulin. That never worked for me.
If you have a good endo, he/she should be able to help. All I currently have are glorified prescription writers. The NP I had been seeing finally admitted she can’t help me with any of problems. So I’m only going in once a year.
Good luck and God’s speed finding something that works.
Hi, i also Have Dawn Phenon but it starts at 11 pm before bed. I have taken bolus at that time because I don’t want to go to bed with 350 BS. That is risking low BS and early in am. My alarm has gone off. But otherwise I wake up with high glucose..(like 275) after sleeping 8 hours…..it’s scary.
When I take the bolus and my Tresiba at night i wake up with a 120 or so. I have yet to talk to an endo about Dawn Phenon..(read my post about new endo) or how to counter it. I have only my web searches on the topic…and some ideas on reducing it. Also we can both read the web link John gave you.
@MikeR1 Thanks for the tip on statins. I’m looking into it although a quick search turned up mixed messaging, some prescribing information sheets have a note and others don’t. I definitely have to look deeper.
@Andrea8 11pm is too soon for DP unless your body’s internal clock isn’t synced to sunrise anymore. The other thing that affects DP is time since your last meal. I included a whole 24 hours from my CGM so you can see an example, dinner was a little after the 7pm bolus, my carb counting was off so I knew I needed a correction by 9. How early are you eating dinner?
I go to bed about 12:30 am or 1:00 (probably a problem)….I often eat dinner at 7 or later. Even when i bolus for the carbs at dinner it seems my BG goes high after 10:00pm. Even if I do a correction for anything else I may eat.
I know it happens in non-diabetes but they produce insulin to counter it. I have had frequent high glucose near bedtime for my 3 years of diagnosis. I may not be synced to sunrise as I get up at 8:30-10:00 am.