I’ve been pumping Fiasp for a week now and am LOVING it. I’m just getting to the stage where I’m going to do some basal testing, and since Fiasp is SO much faster acting than Apidra was for me, I wondered what basal rate delay others are using. For Apidra I made a basal rate change two hours before I needed it to kick in, but I’m thinking of using only an hour with Fiasp and wondered if anyone else had had success with this timing.
1 Like
Today I am seeing a blood glucose change about 1 hour after the basal rate changes with Fiasp. So I am using 1 hour.
With Humalog it was between 1.5 and 2 hours.
When I do some detailed testing I may change my mind but I am going with 1 hour for now.
1 Like
Jen (and @AE13) , do you do a formal basal rate testing protocol or just make changes and watch your CGM?
I’m so jealous! I was told it was not approved for pump yet.
It’s not, but you can still use it to pump “off-label” if your endo is okay with it. My endocrinologist says the studies of using Fiasp in a pump are done, they just haven’t been published yet.
2 Likes
My endo also did not give guidance for when to change basal rates and said the Fiasp pump study is coming out soon and he could not give advice on pump use until it was published. He assured me I would figure it out 
@Terry4 I lead a busy life so I usually set basal based on the CGM but will do a more formal test when I have time and can put up with not eating. Since starting Fiasp I have only tested overnight basals and up to late afternoon. I had to shift a moring rate change 1 hour back.
In diabetes ao much is varible so it is hard to have a controlled experiment… but I have noticed since switching to Fiasp I am moving towards a more constant basal rate across the day. I used to have a morning peak and an afternoon valley, now it is pretty constant all day. I need a bit more time to experiment though to see if I am just imagining things.
I’ve actually moved to making basal rate changes based on BG traces from my CGM. I don’t do fasting basal rate setting anymore.
Stephen Ponder (Sugar Surfing) liked a single basal rate when he was on a pump. Since I started using a hybrid AP, I have my basal rates down to four segments ranging from 0.6 to 0.9 units/hour, the flattest basal profile I’ve ever used.
I’m curious to see where you and Jen and others take using Fiasp in a pump.
1 Like
When I’ve had large changes in therapy, I tend to do a series of fairly formal basal tests. The last time I did this was two years ago when I started the CGM, and I think it’s a big part of why I subsequently had the lowest A1c levels I’ve been able to achieve. I’m not ultra formal about it, because there really are too many variable at play to ever get a perfect basal, but I do skip breakfast, lunch, and dinner twice over a couple of weeks to make changes. I do also change basal rates regularly based on CGM data.
Oh man, I so want this for my daughter - but it’s not approved for under 18 yet in Canada.
Love hearing your updates… keep them coming!
Terry - could you talk about this more? What do you mean by “BG traces?”
Ask her doctor, you may be surprised. It’s not approved for pump use either but my endo had no issue with that.
1 Like
I could have provided more detail. Instead of fasting as called out in the typical basal testing protocol, I watch my CGM lines (BG traces) for a pattern that suggests a needed change in my basal rates. I rely almost totally on the Dexcom Clarity 14-day standard day report. If that report shows a pattern that breaks my upper or lower limits and I can see a meal is not involved, then I’ll make a basal rate change.
For example, if the Clarity report shows a pattern of going low just before I wake up, then I can be confident a basal rate needs changing. I make that change about two hours before the pattern of lows. I’ll look at anything identified in the Clarity report showing yellow for high or the red for low as a “pattern.” The Clarity threshold for identifying something as a pattern is higher than my personal threshold. If I see red or yellow in the 14-day report, I will be taking some kind of action, basal, bolus, better food choices, or exercise.
I see. Thanks. I find Clarity’s ability to self identify trends very modest.
It is rare that I ask Caleb to fast. I look for opportunities when it naturally happens. I think it’s worked out so far. It’s so hard to hit the moving target - we get tight control, then thinks change, tweak and repeat, repeat, repe
For those interested:
The week before starting Fiasp I had an average over the week of 8.4 mmol/L (151 mg/dl), standard deviation of 3.9 mmol/L (70 mg/dl), and time in range of 52%.
The first week of using Fiasp I have an average over the week of 6.9 mmol/L (124 mg/dl), standard deviation of 2.4 mmol/L (42 mg/dl), and time in range of 60%.
Zero change in diet.
3 Likes
I’m trying something new with Fiasp where I am lowering my carb ratio from 15 to 13g covered by 1 unit of insulin. With NovoRapid I would have lows later on if I lowered my ratio below 15, but would have to use the superbolus technique with almost every meal to have enough insulin up front and avoid big spikes. With Fiasp I am still using the superbolus often but am finding I am getting highs later because of the shorter tail. I am wondering if lowering my ratio will give me enough insulin up front without a later low due to the shorter tail.
Ok - My laugh for the day. Yesterday my Omnipod started screaming at 9am. This is my first ever scream failure. I did not have a back-up pod with me, so I had to make-due with my back-up insulin pen for the day.
I spent my lunchtime on the phone with Omnipod learning a -106 alarm was an occulusion alarm, so that was the perfect opportunity for an afternoon basal test as I did not eat lunch.
I know the “rules” are give a shot every 3 hours to make-up for the missing pump basal, but hey, my rate is 1 U/hr right now, so I just gave a shot every 1 hour. Well of course not exactly one hour because I was talking to someone or in a meeting so would ignore my 1 hour time, but close enough. CGM trace looked pretty good all things considered.
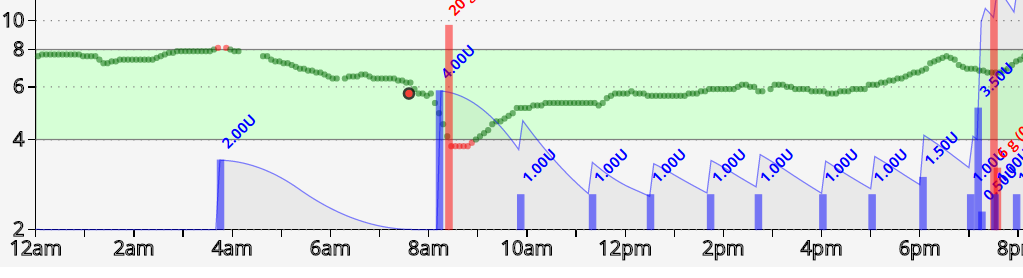
(4=72 and 8=144)
A couple of points:
-There was a Fiasp correction just before 2am when my CGM alarm went off. You can see that most of the lowering action happened in 2 hours then it was pretty flat without much tail.
-The drop around 8am was caused by a shower. This happens - it is part true and part CGM problem.
-It looks like I need another basal segment to correct the rise that starts around 5pm. I have been noticing this on my CGM 7 day average.
Not a bad day all things considered.
2 Likes
Nice way to frame this difficulty as an opportunity instead of a diabetes nuisance! Your workaround ended up working well. I’m curious, did you prime your pen for each one unit dose? If so, how much?
I prime for small doses. Usually 1/2 or 1 unit - enough to see something come out of the pen needle. I use a 1/2 unit pen.
I got out of the priming habit a while back when I gave large boluses. I got back into the habit when my son was diagnosed with T1. 100% of his doses are less than 1.5 units so accuracy becomes important.
I thought readers following Fiasp might find this report interesting. Tim, on his Diabettech blog, is an early adopter of Fiasp. In the linked report he summarizes his experience using Fiasp at 60 days.
While his experience with Fiasp is combined with his hybrid closed-loop system, he provides some interesting observations about changes he’s made with respect to insulin sensitivity factors, insulin to carb ratios, and duration of insulin action.
2 Likes
Thanks for the report. I’m a month into using Fiasp and I had a slight increase in insulin sensitivity. I’ve also moved my DIA to 3.0 hours (with Apidra it was 4.0 hours). I’ve also noticed that sites do not last as long (for me they went from lasting 24-48 hours to lasting 12-24 hours or sometimes even less, though with steroids most seem to last 48 hours) and, even when they do, they often have a lump. I’m not sure what causes this.