Tight blood sugar control reduces the risk of developing microvascular diabetes complications. The evidence of benefit is mainly from studies in younger patients at early stages of the disease. Benefits need to be weighed against risks including severe hypoglycaemia, and patient training is an important aspect in practice. The effects of tight blood sugar control seem to become weaker once complications have been manifested. However, further research is needed on this issue. Furthermore, there is a lack of evidence from RCTs on the effects of tight blood sugar control in older patient populations or patients with macrovascular disease. There is no firm evidence for specific blood glucose targets and treatment goals need to be individualised taking into account age, disease progression, macrovascular risk, as well as the patient’s lifestyle and disease management capabilities. ~~ Intensive glucose control versus conventional glucose control for type 1 diabetes mellitus.
Great - that’s about as good as it gets! Thanks for sharing your thoughts about temp basals. I’ve had couple of 3-4 day long trips recently and have noticed changes in the opposite direction - had to do some more carb nudge corrections. In my case, this could be related to changes in time zone and/or altitude - who knows. In any case, I’ll keep such extended temp basals in mind for upcoming trips.
Thanks for the comment, @Dragan1. I’ve primarily used temp basal before for exercise mitigation. What surprised me with this experience was the extended period of 12 hours or so. In sugar surfing terms it’s kind of an extended nudge. It makes sense that illness can increase insulin resistance and require a bit more insulin to overcome it.
To clarify what I believe the quote means, the book uses the terminology “lower half of that range” Here’s the math spelled out 200 - 65 = 135. Half of that range,135 is 67. The upper half of that range is 200 to (200-67) while the lower half of that range is 65 to (65+67) or 200 to 133 and 65 to 132.
Intellectually, in terms of philosphabetes, there’s a difference between “goals” and “targets” as they play out in our BG. As I see it a “goal” is the range (70-130, 100-200, whatever…) while the “target” is what a pump is set to calculate adjustments at, if BG is up, the small corrections are calculated and, if it’s down, they are cut. Unfortunately, I don’t recall what my original targets or goals were to compare (nor, seemingly, do I recall my username/ password for CareLink as it’s been a while since I got in…hmmm…) but using a somewhat lower range and setting a tight, narrow target seem to have helped me get my BG/ A1C where they are, despite eating more carbs and while having been pretty active running, lifting, etc.
I don’t want to say “diabetes is a game” but maybe I do. If we make it a game, other terms that are applicable to games can fit what we do to. Practice, winning, etc. I am demented enough philosophically to accept a “bad” number as an opportunity to “win” by doing a good job fixing it. Perhaps a psychologist would have a field day exploring how that is disordered but I am not seeing a psychiatrist any time soon.
Thanks for the correction. I misread the meaning of the word target in some of the post. The definition you posted makes sense in that context.
My Accu-CHEK Aviva Combo target range is currently set for between 70 and 100. The Accu-CHECK won’t allow the top end target range to do below 100. I’m willing to experiment a little but I’ll move the bottom end target down to 65 first. I’ve been getting a lot of hypos and with my busy schedule I don’t have time to spot check the Dexcom every 10 seconds to adjust for any predicted hypos. And when I do get one, it leaves me wiped which doesn’t make for a productive work day.
I think stress hormones which may be secreted during illness is one of the causes of hyperglycemia as well as medicines, such as steroids and diuretics.
Great numbers, Khurt! I like the standard day presentation, too. At one glance you can see the time of day that needs attention.
I only use one “target.” It is 83 mg/dl because I think that is the perfect blood glucose number. Like an archer, I shoot for the bulls eye. But my target number is only used when I correct. I’m more than happy when a high percentage of my CGM dots end up in my range. As @acidrock23 said, this has more to do with goals.
I also like the Clarity software and its calculated A1c number for the chosen date range. Clarity uses the standard day, too.
Very good results @Khurt_Williams. Wish you success in taking care of the evening highs. Also, thanks for pointing to Diasend - have not used it before - will check it out.
Finally, a flatline that’s more than three hours long to share! It’s not much, but it still feels like a victory right now. I’ve been fiddling with my overnight basal rates for the past week trying to achieve this.
One thing I’ve learned is that, even after “setting things right” good control doesn’t just happen. It’s a constant adjustment and re-adjustment, both in terms of re-adjusting basal rates and ratios and in the “Sugar Surfing” sense of dealing with highs and lows (or potential highs and lows) as they come up.
Lately I’ve felt like my blood sugar has been a lot more volatile than it was back in the spring when I first started the Dexcom. But I got my A1c on Saturday and it was 6.2, so I’m still managing very well. It’s amazing to me that I spent 23 years with fewer than ten A1c results below 7.0, and only two below 6.5 (both 6.4, due to lows), and in the nine months since I’ve had the Dexcom my A1c results have been 6.1, 6.0, and 6.2. The knowledge has been life-changing, but just as important to achieving those results has been acting on the knowledge and experimenting to see what works and what doesn’t on an ongoing basis.
To remind myself of how constantly demanding diabetes is, and save myself the frustration that I sometimes feel, my new mantra has become, “I’ve got it!..And don’t be surprised if it changes again in the future.”
Great A1C results, @Jen, and a nice flatline pictured here, too!
Your A1C results remind me (along with getting my A1C blood draw today), that A1C is the very blunt instrument that provides a metric on how well we are doing. Time in Range is a more precise measurement, and I have been way off my personal best in the last month … back to the work of getting my TiR better.
Yep, me too. In the spring my TiR was around 70%, and lately it’s dropped off to 50%. I’m not exactly sure of the reason for the volatility, but I’m hoping to improve it as well.
Awesome flatline @Jen, congratulations! I share your sentiment - the feeling of being in control is even more important than any numerical result. As you experiment more you get better at it, and I am sure you’ll be able to improve your TiR and A1c further - keep us posted.
@Jen, great work. I share your sentiment that reining in diabetes is an ever changing task. Your depicted flatline is no fluke! It is the result of a concerted and overall effort to control your blood glucose.
The idea that a perfect basal rate, insulin to carb ratio, and correction factor exists impairs our thinking about diabetes. Once you give up that idea, it grants one permission to shoot at the moving target knowing that this is the reality of dealing with diabetes, not the aberration. I now look at my pump settings as getting me in the right neighborhood. They put me on a platform close enough so that I can make dynamic changes with a better chance of success. When the platform moves out of that zone it’s my job to move it.
Stock market investors are warned to not get emotionally attached to any specific stock. Doing so places you at risk of “marrying” that position and clouding your judgment when market forces move against “your stock.” Instead, success pivots on understanding the reality of dynamic forces. Investing in stocks and appreciating and using diabetes data share similar traits.
I agree with @YogaO about the time in range statistic. I think it is the king of all diabetes statistics. It is built on reaching for flatlines day after day after day.
The reason I remain enamored of flatlines is that so many forces are arrayed against it. Yet we can, from time to time, counteract every one of those many forces and make diabetes do what we want it to do. Incredible!
I like the flatline because it sums up, in one image, all my hard work better than anything else can. It’s also something that non-diabetics can relate to when I’m trying to explain the huge benefits of using the Dexcom compared to not using it (I would never be able to flatline without the Dexcom!).
I feel like at this point my biggest challenge to TIR are monthly hormones and similar changes in insulin sensitivity. Yesterday, after posting my flatline, I proceeded to run high all day and only came back down when I upped my basal rate by 0.2 and upped my ratios from 1:10 to 1:8 and 2.0 to 1.5 mmol/L. Then, overnight I went low (probably from stacking insulin throughout the evening), and after treating that I was flat the rest of the night. Hopefully today will be better, but I always have to be on my toes for moving my basal rates and ratios up or down by a fair bit, and this is where I find that even Sugar Surfing fails. Because I never really know whether this is just a “regular” high that will come down with a correction or whether it’s one that will need me to put my basal and correction ratio up before it’ll budge, I have to wait several hours to see what it’ll do before making any decision.
I’ve started to try to work out some clues that will let me know the reason behind the high, but it means running high for several hours. For example, if I’ve done a correction and continue to creep upwards past 14 mmol/L (250 mg/dl), that’s a bad site (this happened just yesterday or the day before, even though I use metal sets). If I correct twice and it doesn’t budge but is not going any higher, then it’s basal. If upping my basal doesn’t bring it into range, then I up my correction (and carb) factor and correct again. If that doesn’t work (or it works but I go high again shortly thereafter), then I up both my basal and ratios a second time. This i the process I went through yesterday, and it worked, but meant running high all day. But I feel adjusting settings any faster than that is too fast.
I’d be very curious to hear how women who have a low A1c and high TIR manage these types of fluctuations. I’ve gotten good at managing changes in schedule or unexpected things like having to walk 25 minutes home because I’ve missed the bus, which is great. But the big shifts continue to hinder me.
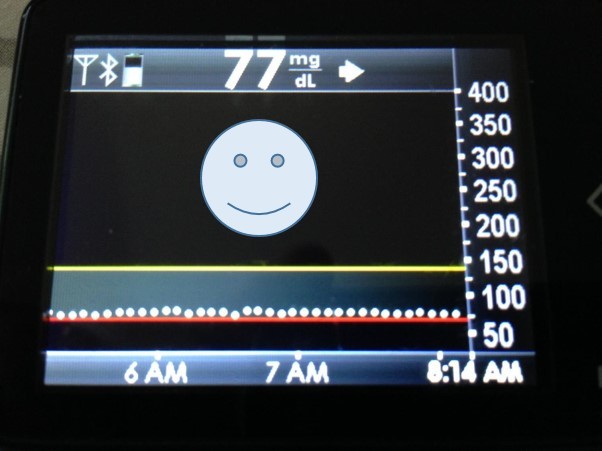
It does not take much to make a person with T1D genuinely happy (at least for a moment): some white dots nearly perfectly aligned just above a horizontal red line on a dull little screen. And they say there is absolutely nothing good about living with T1D? Nonsense!
I love it when that happens! Like dots simply ladled onto an abstract plane of perfection. There are 92 reasons why this should never happen and you denied each of them their penchant for chaos. Call me crazy but I take pleasure in lines like this. Well done! Look no further, this is the antidote to diabetes blues
Just to make this clear: the literal flat line is an exception, does not happen very often. It is a coincidence in the same sense as when a bg meter and a CGM show exactly the same number at the same time. Plus, during those hours I really did not do anything at all - I was just happily sleeping. Obviously I had made some effort in adjusting my basal rates, which in my case is almost 3 times higher in early morning hours compared to late afternoon.
Me too! I still remember the times when I was, as a newly diagnosed teenager, testing for sugar in urine by dropping a tablet into a tube and waiting, in anticipation, for the chemical reaction to end, and then feeling tremendous joy if the color turned blue (indicating no sugar in urine). Technology has changed over the past 40 years, but I guess I have not changed my attitude towards T1D that much. I’d say better ‘crazy’ than feeling guilty or depressed about it. Wish ‘medical professionals’ understood the importance of positive attitude and motivation better than they seem to do, but that’s a different topic.
 200 - 65 = 135. Half of that range,135 is 67. The upper half of that range is 200 to (200-67) while the lower half of that range is 65 to (65+67) or 200 to 133 and 65 to 132.
200 - 65 = 135. Half of that range,135 is 67. The upper half of that range is 200 to (200-67) while the lower half of that range is 65 to (65+67) or 200 to 133 and 65 to 132.