Nice touch - even the Dexcom’s happy! 
Yesterday wasn’t bad for me - not up to your standard (heh), but definitely a “Between the Lines” day:
Nice touch - even the Dexcom’s happy!
Yesterday wasn’t bad for me - not up to your standard (heh), but definitely a “Between the Lines” day:
@Thas - Excellent! Your line looks like a standard deviation of about 15, non-diabetic.
Seems there’s a rash of flatlines breaking out around here. I had a good day two days ago.
Great work folks! It’s great to see people who are getting things in control. There are many threads, posts, memes, etc. saying “diabetes can’t be controlled”. I’ve always sort of rolled my eyes at them but this group of people from around the world are doing it regularly. The dialogue here is really amazing too. I’m off to the endo today and am not optimistic about hitting 4.9 again although, as is often the case,things seem to tighten up a bit right before then 30 day avg is 100 w/ 81% in range (70-130), Std.Dev 24.9 vs. 7 day avg at 97 with 89% in range, 5% hi and 6% low, 18.2 Std. Dev. Meter BG average is 108 but that’s always higher as I don’t bother inputting low BG into my pump so it skews that that way.
Unfortunately, I’m running a bit late this AM so I don’t have time to do pics and had to eat…CEREAL for breakfast, which will be peaking right about the time they are drawing the blood. Or, almost, the post cereal nosedive will be hitting?
A flatline is a great goal but not a realistic one
I went to a presentation last summer by the author of Sugar Surfing, Stephen Ponder. He made a comment about flatlines that caught my attention. I can’t repeat it verbatim but the jist of it was the only people that make flat BG lines are dead! I understood the sentiment even if I don’t agree with its literal meaning.
It’s true that people without diabetes have blood sugar traces and trends that are not level or flat. Mother Nature does not work that way. Homeostatis keeps blood sugar within a relatively tight range of blood sugar. It does not, however, draw flatlines.
I’ve accepted this cognitive dissonance given the namesake of this forum. I know that the real prize for people with diabetes are blood sugar traces that are more normal, not really flatlines.
But we all know however what our blood sugar lines look like if we just give up, eat whatever we want, get careless about our insulin and medication regime, and exercise sporadically, if at all. If we wear a CGM under these circumstances, we see profiles of the Rocky Mountains or the Himalayas. Tall spikey mountains and even deep cut canyons. Metabolic chaos accompanied by foggy brains, mind-numbing lows, and a low quality of life.
So the term “flatline” is really just an ideal, not something we aspire to for 100% of our metabolic life. In essence it means striving toward flatter BG profiles, not necessarily flat ones. It’s an unfortunate semantic side effect of aiming for the truly unattainable perfection and settling for the less than perfect but acceptable lines.
What surprises me, however, is that sometimes we end up with actual flatlines, an unnatural phenomena that even people without diabetes don’t usually experience. Oh well, that’s just the nature of most goals. It’s better to shoot for the perfect bullseyes and just hit near the target than to not aim for anything worthwhile and not even hit remotely near the target. Does that make any sense to you?
[quote="Terry4, post:289, topic:22716, full:true"]
I went to a presentation last summer by the author of Sugar Surfing, Stephen Ponder. He made a comment about flatlines that caught my attention. I can’t repeat it verbatim but the jist of it was the only people that make flat BG lines are dead! I understood the sentiment even if I don’t agree with its literal meaning.
[/quote]
He says the same thing in the book. And I’ve said something along the same lines, myself. I’d be curious to see a weeks’ worth of CGM lines from someone without diabetes – I suspect they, too, will have period where it’s nearly flat, as much as they will have normal fluctuations. In any event, as has been said before in this thread and others - the important goal is to maximize time in range, which seems most likely to deliver the best long-term results…
Or, as I like to say: I try to live my life “between the lines.”
Ponder’s comment (which is repeated in the book) is a good sound bite and makes a good point in the context of sugar surfing techniques, but is a bit imprecise. In steady state (homeostasis), when undisturbed by meals, e.g. during nighttime, healthy individuals have remarkably flat bg lines with very small variations around 80 or so. There is nothing unnatural about near-perfect flat lines for extended periods of time. Of course, they do spike some after carb-rich meals, and do not maintain literally flat lines all the time, which is the point of Ponder’s comment.
I don’t necessarily have the “line” as the goal, as I don’t aim at a line. It’s being engaged enough to approach every test as a chance to have a result that’s on goal or to contemplate putting it there. Sometimes it might take taking the dog for a walk, other times it might need two or three jelly beans. I think that the thing having a tight target does is to help you get engaged. Occasionally, people will suggest “that’s a lot of work” but, once you get into it, I think that it’s much less work than when you aim at 150 and the number ends up being +/- 80 mg/DL in the absence of focus and a CGM to keep it on a short leash.
Missing questions which I would like to see medicine approach formally are 1) does a lower A1C, say <6.0 or maybe < 5.5 (or maybe investigate both?) lead to any positive result and 2) is a lower A1C, as is often suggested, dangerous? It strikes me as unfortunate that a tool like an AP seems more likely to be rigged with the alleged “saftey first” perspective that would lead to more like 100-180 targeting than 85-90 or straight 85. The other question would be where do you put the target for kids who are managed by 3rd parties to varying degrees and have seemingly much more volatile BGs reported. Concerns about safety are very real for CWD and their parents. Then again, how much volatility is caused by overtreating sticky hypos? Dr. Ponder is a pediatric endo and has several pages on FB where we can follow his work and it seems that kids and their parents can also benefit from Sugar Surfing but, in the absence of a formal study, the conclusions of those of us Surfing away seem to be speculative.
I also think this is unfortunate. But I still remain hopeful that once the AP can demonstrate great control in the 100-180 channel, it will only be natural to seek to improve it to say 80-140. My experience with many clinicians over the years is that they are way too concerned with hypos and would easily trade away better control with moderate risk of hypos for poor control with almost no risk of hypos. I’m angry with this position and have totally rejected it as nonsense for me.
Now I know that the docs witness the aftermath when we literally crash and burn with severe hypos. But this is not a binary choice doctors make. There is a middle ground that many of us here have found. We can reduce BG variability and allow us to reduce average BG without increasing time spent hypo.
Even though my endo sees the voluminous data that documents my case with 288 CGM dots every day, her eyes always seem drawn to the 2-3% of the time I am low. And 2/3 of this low time is north of 55. This is completely acceptable to me because my lows are approached with a gently decaying line that gives me lots of time to easily treat with a few grams of carbs. The docs’ hypo-phobia is so ingrained that their reaction is reflexive. Her heart is in the right place and she is very good on other issues so I just bite my tongue and move on.
I completely agree with you. My experience with various endos and nurse practitioners has been exactly the same. They have been trained to assume that better control automatically leads to greater chances of severe lows, which is complete nonsense. I’ve recently made an attempt to teach my endo what I’ve been doing, and she showed absolutely no interest, parroting instead some >20 year old ‘recommendations’. Presenting extensive CGM data to prove that I did not have any severe lows made absolutely no difference to her either. Well, they sign on my prescriptions and order my labs - that’s all I am expecting from them these days. Sorry for the somewhat unrelated rant - it’s just frustrating.
A insulin-only AP (CGM+pump) operating completely autonomously will simply never be able to better than around 100-180 range, because otherwise the safety risks associated with lows would not be just perceived but real. This would still be a very useful system and a step forward for CWD, and adults who have more severe troubles with control. On top of that, I am pretty sure such AP systems will allow ‘hybrid’ action, i.e. user interventions such as pre-bolusing etc. Such a hybrid system, in combination with sugar surfing techniques, could be a winner for everyone. The dual-hormone (insulin+glucagon) AP should ultimately be able to do better than anyone of us can do manually, but such systems are probably >10 years away.
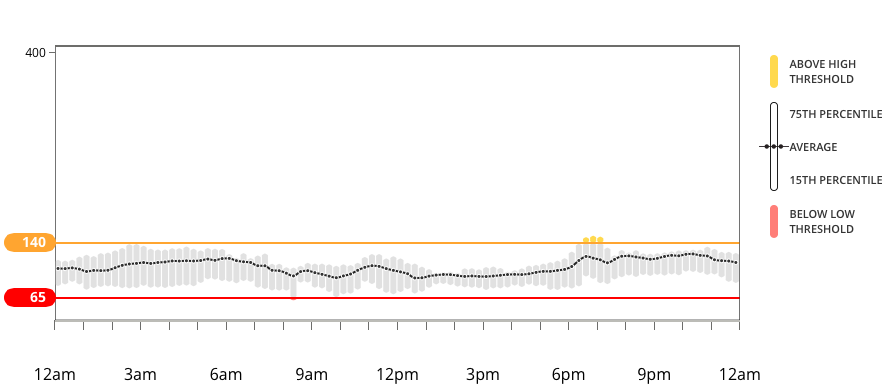
The Dexcom Clarity 14-day standard day is now my go-to report to manage my diabetes. It is very helpful when making changes to my basal rate. The graph below shows a recent 14-day period. While the current status is very good, in the last month my trends varied from overnight lows to overnight highs.
This graph allowed me to flexibly respond and make the basal changes without too much time elapsing. The beauty of this graph is that when the 15th percentile pierces the lower threshold or the 75th percentile crosses upper threshold it’s a solid indication to make a change. In other words it distinguishes between a trend and a less frequent BG aberration.
I am aiming for a meandering path through gentle hills and vast valleys ![]()
An in range sine wave works for me.
@Terry4, @Dragan1 unfortunately neither Diasend or Clarity worked after I updated to OS X 10.11 (El Capitan). Both companies promised an updated driver but … it’s been several weeks so I guess my days of charing my numbers with those apps is over.
PS.
I’m riding a very tight flat line all morning.
That’s good to know - thanks - I was just thinking about updating my Mac to El Capitan - will postpone that. BTW, that’s a cool looking flat! Have a skittle (1g) - bring it up a notch - probably around +5  .
.
Nice! If your Dex is behaving like mine, that 65-72 line is actually something like 75 - 85 and no correction is needed.
My Dex alarmed me twice last night for lows. The first one Dex had me @ 58 (I had my low alarm on @ 60, forgot to turn it off), but my fingerstick was 85. I calibrated and two hours later, it alarmed with a 48, but my fingerstick was 77. (Yawn!)
@Khurt_Williams, thanks for the warning about El Capitan operating system update. I use Clarity every day and Diasend a few times per month. I’d rather wait to update my iOS and still be able to use those two programs.
Nice three hour line. I don’t correct a low line until I fingerstick and verify that it is indeed under 70. I don’t consider an actual low until it’s under 65. I currently use Tic-Tacs to carb nudge.
Good work!
Good point! I suspect that on the low end Dexcom is slightly biased to display values lower than the best estimates. If so, this was probably done so that they could claim better % results in not missing lows, which is important for FDA approvals and comparisons against the competition. Somewhat like a Volkswagen-style software trick? Does not matter - lets not demand immediate recalls ![]()
[quote=“Terry4, post:289, topic:22716”]
So the term “flatline” is really just an ideal, not something we aspire to for 100% of our metabolic life.
[/quote] Correct, Terry. When I named this group several (2010/2011) years ago, it was all in good fun. Something to catch peoples attention.
Be well. Danny
What @YogaO said. I’ve seen long periods where I coast between 65-70 for hours. Bringing that up 5 points means eating … what?