The problem
I’ve been working on adjusting basal rates on my pump to counteract lows occurring in the midnight to 2 a.m. timeframe. These lows are not like any I’ve had before. These are lows that resist added glucose. Let me say that again, these lows don’t respond when I eat glucose tabs!
When this started happening, I couldn’t accept this reality. It’s been a basic law of my diabetes metabolic life for over thirty years. When I go low, drink some juice or eat something fast and carbby and 15-20 minutes later, my metabolic ship rights itself.
It typically happens a few hours after I go to sleep. My practice is to eat my last meal in the early evening so that could climb into bed with very little to no insulin on board (IOB). At the most, I might have less than 1.0 units IOB. Then, after midnight, my CGM would vibrate with a 70 alarm and shriek with an audible alarm soon after. I bleery-eye rollover and check the CGM number. It says 68 and a slight downward trend, a sideways arrow but the dots are marching downhill.
Mystery deepens
No problem, I told myself, just pop a Dex4 glucose tab and roll over. Fifteen minutes later I get another sub-70 alarm and now I’m down to 62. WTF??! OK, mysteries happen. Pop another Dex4 and try to get some sleep. Fifteen minutes go by and now I’m hitting the obnoxious 55 alarm. So I get up and fingerstick, thinking maybe the sensor has drifted off. Nope. Fingerstick comes in at 54. So I eat two Dex4s; that makes 4 total for the episode and I’m baffled.
My last meal was more than 6 hours ago and even with a duration of insulin set at a conservative 5 hours, I’m showing no IOB. I didn’t do anything unusual exercise-wise and I didn’t drink any alcohol. Fifteen to thirty minutes later my CGM complains again; now I’m down into the 40s! The episode duration now stretches to over an hour, I’ve thrown over four glucose tabs at the low and it stubbornly resists. So I eat two more tabs but also get up and chase them with a glass of water.
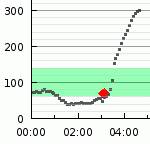
Finally, after about two hours, my BG turns around. But it turns around with a vengeance and skyrockets to 300. It’s as if all my glucose tabs were held behind a dam and let go all at once, too late and too much. Here’s a graph of the action:
I decide to get up and deal with this
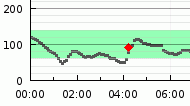
The first lesson I draw is that I need to physically get up when this happens. I need to drink water with my glucose tabs and don’t go back to sleep until the low is neutralized. A few nights nights later it happens again:

This time I do get up, treat with repeated glucose tabs and drink water. I also start adding insulin to counteract the glucose corrections. It took me over an hour but things turned out better. I eliminated the big BG bounce.
Maybe the basal rates are too high
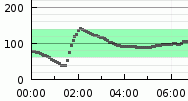
So I start adjusting the 10 p.m. to midnight and midnight to 2 a.m. basal rates. The next night I’m rewarded with this trace:
I took a glucose tab or two and my BG responded. I didn’t need to physically get up. Progress. Here’s the next night:

So things are moderating but I still have that post midnight downtrend. The green strip ranges from 65-140 mg/dl. So that quick jump from the bottom to the top of the range is a mid-sleep glucose tab and its response. Things are getting better but my goal is to sleep through the night with no interventions and a good steady in-range BG line.
In the eye of the storm, a no-hitter
Finally, I’m rewarded with this 24-hour beauty yesterday:

It’s back
So, I conclude that I just had some out-of-whack basal rates and that’s the reason I had those hard-charging lows. But last night, a wrench is thrown into that hypothesis:
My basal rate was unchanged from the good day before. I went to bed with little to no IOB. I actually omitted my usual evening walk. Same symptoms that started this mystery. Woke up to the 70 alarm, took one glucose tab, no response, took another followed by the 55 alarm. CGM went down to “Low” or under 39 mg/dl but fingerstick showed 48. I got up and took a few more glucose tabs and also took two units to counteract the expected rebound.
I’m going to pick up a glucagon emergency kit so that I can mix up a mini-glucoagon shot if this happens again. I’ll take 15 units measured with an insulin syringe instead of the big dose in the kit. I’ve done this before with good results.
Two hypotheses
So, what the heck is going on? I have two theories. The first is that the lower valve in my stomach is not opening and holding back my glucose tabs. I have gastroparesis, so that is a possibility. The second is that my liver stops putting out its usual drip of glucose. Kind of like when I drink a few glasses of wine and the liver gets preoccupied processing the alcohol and the usual liver glucose drip is interrupted and I go low in the wee hours of the morning. I’ve witnessed that event many times.
I’m baffled. I’ll go to my endo next week but I don’t expect much enlightenment on this issue. I’m on my own. Any comments?
