I’m so confused. What is considered a bs spike? I’ve been testing my bs 2 hrs after a meal. My understanding is that if I’m 180 or under at that point I’m good to go. But, what if I test at 1 hr and I’m 260 and then test again at 2 hrs and I’m 190. Is that 260 considered a spike? Is it ok to “spike” to any number after a meal as long as by 2 hours you’ve come down to or near 180?
My understanding is that a spike is when you go outside of your target range. Without a CGM it could be very difficult to manage that. If you do have a CGM, then you may be able to time the bolus with your meal spike to essentially cancel them out. Otherwise, there are charts such as the one below that specify targets around 1-2 hrs after meals. Homeostasis in your target range is the key, I think.

3 Likes
generally I don’t look at the 2 hour bg. I might check my bg at 3 hours post prandial, but even at that time, there’s still IOB for the meal and any corrections could lead to stacking.
3 Likes
I don’t know if you pump (and which pump you use if you are a pumper), but the “bolus wizard” on your pump should take into account the insulin on board in a decreasing fashion as you approach the time you set as your DIA (duration of insulin action) in settings in order to prevent insulin stacking.
For example (I’m using the OmniPod system as my example, as that is what my 13 year-old daughter uses), let’s say my daughter forgot to bolus and ate a ginormous Cookie Dough Blizzard at Fairy Queen. About 20 minutes later, her Dexcom starts screaming at her because her BG just topped 170 and is showing double arrows up. But she selectively doesn’t hear the alarms until it becomes too bothersome to ignore them, so she checks and her BG is now 368 with double arrows up. (Yikes! I cringe when this kind of thing happens!) So she grabs her PDM (“The Brick”) and inputs her BG of 368, and the bolus wizard recommends a correction dose of two bazillion units. She goes for it and her trusty Pod delivers the correct amount of insulin. An hour and a half transpires during which she is in the nastiest mood ever, finds fault with every single word that escapes my mouth, and launches into a loud monologue on why no one should have to do chores until they turn 18 and people should be allowed to drive when they turn 14 and I should buy her a new car and keep our junker for myself, and why won’t I let her get her nose pierced before she turns 16? I have her check her BG and it has only gone down to, say 285, and I know we are in for a very sticky high that will require some rage bolusing. So I input the new and only slightly improved BG of 285 into The Brick. The bolus wizard will show an amount of IOB that is clearly less than the original two bazillion units my daughter bolused an hour and a half ago and will recommend an additional amount of insulin, e.g. one-eighth of a bazillion units of insulin, because it is taking into account the part of the original two bazillion units that is still on board. I wouldn’t expect her to go low after this second bolus because the pump accounted for how much insulin was still on board when it recommended how much of a correction to use for her still-higher-than-expected BG of 285.
Different scenario. It’s 30 minutes until dinner. I help my daughter count the carbs and I tell her to input her current BG and the number of carbs in her meal so her bolus wizard can suggest a bolus amount. But she gets distracted and when it’s 10 minutes until dinner, I ask her if she remembered to bolus. She says she forgot, but does it right then. Well, I want her to surf and wait for the bend, but she is incredibly hungry and can’t possibly wait that long and it’s not fair because I don’t ever have to wait before I eat and it’s not her fault that she has T1D and can she please just wait only 5 minutes before she starts to eat because she will die otherwise. I cave (I usually do when she plays the “D-card”) and I let her stuff her face knowing full well what is around the bend. Instead of going up to, say 175, and then floating gently back down to land at a respectable 103, she is spiking at 220 40 minutes later. Now in this scenario, if she were to input her BG of 220 in an effort to correct, the bolus wizard would recommend a correction of zero because there is still sufficient IOB to (hopefully) correct this high that occurred because my daughter didn’t pre-bolus. If I got to feeling antsy and decided to override the bolus wizard and throw in an extra 1.5 units or so, I would risk her going low because this would be stacking insulin.
5 Likes
I think the 260 would be your spike but it came down to 190 and as the insulin keeps dropping you down you will hopefully go down lower into a normal range. It can vary widely depending on each individual and what he/she eats etc.
People who don’t have diabetes can eat whatever they want to and most of the time end up at 80-90 2 hours after a meal. For the most part I think their spikes are in the 120-160 range or lower for a high carb meal, their bg comes down naturally and rapidly without causing hypoglycemic reactions. And their spikes aren’t so high due to the first phase of insulin.
In general you need to be very cautious to correct a spike when you have significant insulin on board and especially if you’re also doing any kind of activity… If you fluctuate a lot and can drop rapidly you can get into big trouble. I have dropped extremely rapidly from 200 many x and can I easily come crashing down even with no correction especially with activity.
I don’t think it’s ok to spike to any number… for me anyway, I don’t want to spike really high for numerous reasons. First It’s dangerous, you can have a stroke/blood clots and other events, it’s much harder to come down once you get up into that stratosphere and more dangerous to drop it down.
2 Likes
TuDiabetes never gets stale; I always learn something. In this case, a new clinical term: gazillion.
The word spike has no formal definition but I think of it as a quickly elevating BG that often tops out above my “normal range.” Here’s what I’m thinking about:
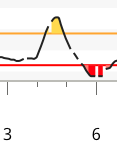
This spike started out at 80 mg/dl and topped out at 178 mg/dl in 44 minutes. In this spike I over-corrected a little but brought the spike down quickly, my over-riding goal. My sensor over-reacted to the post-high low and it really only came down to 66 mg/dl. This spike I think of in terms of looking like Mount Everest, tall and jagged.
Here’s another kind of hyperglycemia that I think is just as significant, but not as dramatic:

This hyper topped out at 200 mg/dl but was out of range for seven hours. I hate it when this happens. I didn’t correct in a timely way due to sleeping through a few CGM alarms. I think of this mountain more in terms of Mauna Loa on the Big Island of Hawaii. It looks much shorter than it really is since its footprint is massive. Mauno Loa tops out just under 14,000 foot above sea level.
Both of these events do their damage. Studies have shown that high BG variability damages your metabolism and tissue too. Neither of these events is desirable but I’d take the short and sweet spike any time over the long enduring slow climb into hyperglycemia.
Statisticians often refer to the “area under the curve” or AUC. In this measure less area is better. You can quickly see that the yellow shaded area in my Mt. Everest spike example is much smaller than the second Mauna Loa depiction.
By the way, I do not let insulin stacking keep me from being aggressive with insulin. This comes from lots of personal experience and observation. If I see a rapidly rising BG, I will dose insulin without fully considering the IOB. I often use Afrezza and/or an intramuscular injection combined with a 20-minute walk to speed up insulin action.
3 Likes
I’ve had some what I call Mount Everest spikes. When I started on my pump, my silly team reduced all my insulin and told me to eat an exact carb low fat meal for a test. I spiked from 110 to 289 in about 20-30 minutes… horrible. I don’t like the fast spikes at all if they’re that high. I can no longer dose for rapid spikes without extreme caution because I can drop like a stone and go very hypo.
Thanks everyone for the responses. They are so helpful.
@rgcainmd - you should be a writer (oh, and, I think our daughters may be twins…)
@Terry4 - from your screen shots it looks as though your “normal range” might be between, about 65 to 140…? I don’t know what my target range is. Would it be the same as yours (is that a typical range?)? Or is it something my Dr. determines? I’m still fairly new to all of this and am realizing that I haven’t had as much education as I may need. I just thought that no matter what or when - as long as I’m near 180 or below I’m fine. My fasting bs was 165 this morning and something I read on here yesterday now makes me think that, that is not ok.
Yeah, I wouldn’t want to wake up to 165 mg/dl for many days. Yes, my target ranges from 65-140 mg/dl. I chose 65 mg/dl as the low boundary because I know I become hypo-symptomatic at that level. The 140 I chose because I’ve read that damage to tissue starts to occur at that level.
Your target range is whatever you set it at! It’s good to listen to the doctor but this is your choice. You know where you feel well and don’t. A relatively tight range like my target depends on low BG variability to stay safe. My levels drift more than plunge. Doctors will often start out with an 80-180 mg/dl target. I think that’s fine to get someone started but those who are capable should seek further improvements.
Reduction of BG variability as expressed by standard deviation will accommodate narrow ranges and increase safety margins. I limit carbs in my diet; it’s the only way for me to significantly shrink variability. I seek my standard deviation <= 30 mg/dl.
I can’t help but comment on what you’ve posted. The correct number of units recommended by my daughter’s bolus wizard was two bazillion units. If I had accidentally given her a bolus of a gazillion units, however, she wouldn’t have lived to tell the tale! 
1 Like
Sorry, I transcribed the wrong term. I stand corrected. (Actually, I sit corrected, but it works out to the same thing.)
1 Like
Is a bazillion more or less than a gazillion?
A gazillion is a kazillion times as much as a bazillion.
Interesting. I usually measure my large insulin doses in “crap-tons”.
2 Likes