While I’ve been using a continuous glucose monitor or CGM for eight years now, it’s only been in the latter portion of that period that I’ve come to appreciate the beauty of this metric. The medical and research community seem slow to fully embrace this measurement and fixate instead on the A1c number. There are definite exceptions to this A1c-centric focus and I think things are starting to change.
The biggest weakness of the A1c is in hiding blood glucose volatility and the extent of hypoglycemia. Unfortunately, it has led some clinicians to reflexively warn about hypoglycemia incidence based on an A1c number alone. Statements by clinicians such as, “I don’t like my diabetic patients to pursue an A1c below 6.0% since that means too much hypoglycemia,” don’t even consider that some of us can achieve lower A1c’s without increasing hypo risk.
To me, time-in-range, is the perfect diabetes statistic. A high percentage of TIR (80%-90%+) inherently means less time both high and low. When I can consistently measure 80%+ time in range, I feel better and enjoy more energy and clarity of mind.
Focusing on staying in my ideal range (I aim for 65-140 mg/dL or 3.6-7.8 mmol/L) means I have to tame blood glucose variability. Variability is the main impediment to lowering average BG and spending more time in range. Lowering variability also means fewer hypos and increased safety.
Adam is an unashamed adherent of the high-fat, low-carb way of eating, something I share with him. This graph hammers home his point.
I encourage everyone to click on the link and read his entire column. He brings experts into the conversation, including doctors like Irl Hirsch who lives with T1D. It’s well worth the read!
Terry- I also read that article yesterday with great interest. It again drives home how we all should have our own goals, not the ones that the ADA thinks or a doctor who thinks everyone is the same.
The in range target is a moving target for me. And like the numbers I use for my in target numbers have changed, the time in range continues to change. As I have learned to use the CGM alarms and the micro dosing with insulin and carbs, the numbers have tightened up.
When and now it’s 180. My standard deviations was 60 I have lowered to 50. I think everything is about learning from past experiences and helping those experiences to keep the out of range from happening again. The last time I saw one of my endos we talked about working on getting the low range a little smaller which would help with the in range targets.
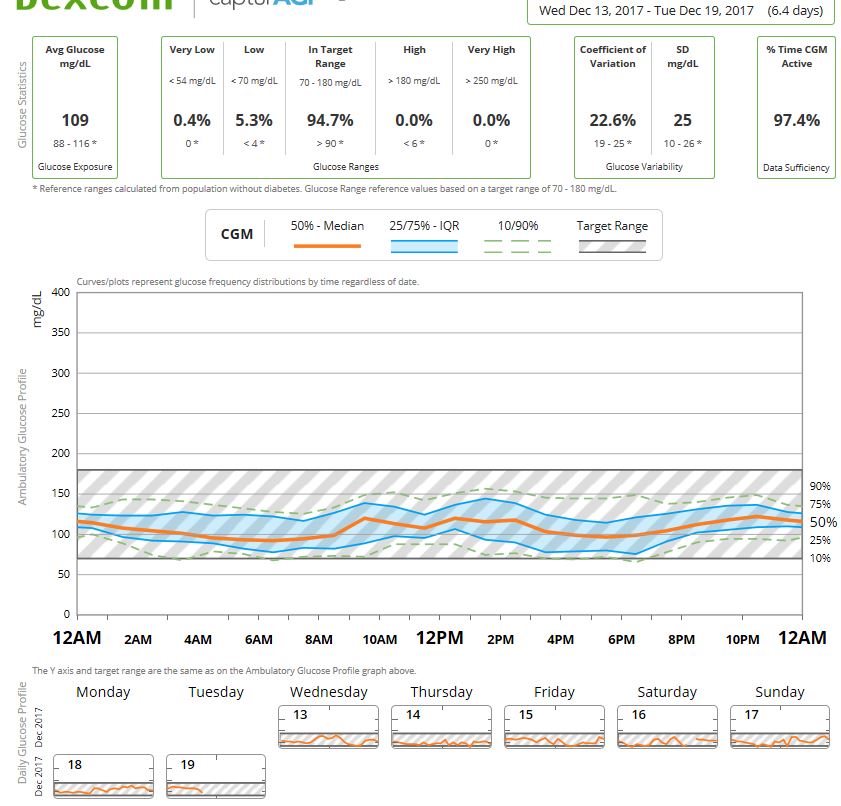
I again am thrilled that people are starting to realize that it is not all A1C. And if you have a CGM going all the time, those numbers will tell. I love the AGP report, it really has everything you need. And that is the report that my doctors spend the most time with.
Each of us have different goal, experiences and life issues that will effect a persons time in range but hopefully people who start to realize that there is no perfect number.
The time in range goal is nice since one can adjust it to her/his circumstance and preference.
I’m impressed your doctor uses the AGP report during your visit. It is a nice and concise one-page graphic that shows a comprehensive view easily understandable for both the doctor and patient.
My doctor’s office doesn’t use it even though the clinic director is one of the signers of a 2013 paper that promotes the AGP as a graphic tool appropriate in today’s busy clinic when the doctor’s time is limited.
Our Endo pulls up both the Clarity and the Diasend online data during our visit. Our Endo visits usually last an hour.
There is very little time spent on A1c discussion. Last visit probably less than 60 seconds. Then analyzing the Diasend and Clarity data looking for any patterns that we might have missed that could be beneficial to make changes on.
I understand the value of A1c when not on a cgm. Just by looking at the fingersticks might not give a good picture as perhaps the fingersticks may often times be done when the person feels like their BG is out of range and needs a correction. Certainly does not necessarily imply what the overall BG is like. Really depends on the person and how often and how many data points they are getting per day.
With a cgm - it just provides far more information. The A1c is a good double check on the validity of the cgm data. If the A1c and the cgm data make no sense with each other than it is a good time to sit down and figure out what possibly is going wrong with the numbers and data collection. But if the A1c makes sense in relation to the cgm than it is the cgm data which will provide the real insight to see where realistic improvements are possible.
It can be, but not necessarily so. Did you know that an A1c of 6.0% does not equal a specific estimated average BG of 126 mg/dL (7 mmol/L) but instead corresponds to a range of glucose running from 100-152 mg/dL (5.6-8.4 mmol/L)? A1c is not as precise as we often give it credit. I’ve found my CGM average does not land at the median or average estimated BG. It usually is lower.
I verify my blood glucose meter with the lab every 90 days so I know that the device I use to calibrate my CGM is reasonably accurate. (to the extent that +/- 10% is accurate!)
I agree that an A1c number, in absence of CGM data, is better than nothing. Unfortunately it cannot give the patient or doctor any info on BG variability, a key glycemia component.
My endo also uses the AGP graph at our appointments. We don’t discuss A1c at all, other than he tells me what it is.
I think the main disadvantage of TIR is that most people with diabetes do not have access to technology that can generate this statistic in a reliable manner (which can only be done by measuring BG throughout the day and night). Here in Canada the use of CGMs is very low (I would guess well under 10%) because most people have to pay out of pocket. With devices like the Libre, hopefully governments/insurance will begin to cover the cost so that more can afford to have access to this type of data. But until then, TIR is really only available to those of us lucky enough to be able to afford to purchase or have insurance that covers a CGM or FGM.
I agree that TIR can only be usefully generated by a CGM. CGMs are only worn by about 10% of T1Ds in the US.
After wearing a CGM for eight years, I’m surprised by how low this statistic is. I realize the affordability challenge faced by many but I also suspect many people see CGM use as more of a nuisance than it is a benefit.
This confirms my growing awareness that my diabetes experience does not represent well the experience of many with diabetes. I need to remind myself how lucky I am with my access to good and affordable health care.
I just got finished with a phone call that also covered thte AGP graph. I found out that it can’t be modified to show TIR for our custom settings. Reading about it explained why, so I have to use another Clarity report to find MY TIR, using a lower high limit than 180.
[EDIT]Terry enlightened me about the option in Settings to change AGP threshold.
Not sure I understand what you mean by this. I know I can change the upper and lower limits to create the range used by Clarity via the “Settings” tab. Scroll down to the AGP Target Range heading. Here’s what it looks like.
Wow, your graph is amazing. If you don’t mind me asking, are you t1, and what is your insulin regimen and technologies in use? I can’t imagine achieving such results as you except with the help of an aps, as @Terry4 uses. I am looking forward to OmniPod releasing is version hopefully this year…
Been T1 since before 1978 (dx was years late in coming. I had gradual onset), lousy A1c for years on the old insulins, and no meter. Some A1c’s were over 9. Eventually got them into the 8’s and 7s. 7’s for a long time. Got a pump (MM) in 1997 and that was the start of the partial reversal of some of my issues like numbness in feet and elsewhere. Also marked the last time I had to have Glucagon (but still have it “in case”). I nearly gave up pumping because of the lousy performance (for me) of cannula sets. They would get kinked so often it was maddening. Switched to steel sets and it’s been smooth sailing with a variety of Medtronic pumps since then (I forget what year I switched to Sure-T’s). My Dexcom is the final piece of the current puzzle to keep my bg’s more level. My most recent A1c was a record for me! 5.7. That was roughly 2 months ago. Usually I’m 6.1 to 6.4 for years on end.
Keep in mind that while I’m new to a Dexcom CGM, I have always used a ton of strips per day (not anymore!). Like around 15 or sometimes over 20, but average 17. I’m too active at times to be doing any 3-4 strips per day nonsense.
CAREFUL carb counting the last 2 weeks has improved my glucose levels so much it’s hard for me to believe. I’ve dropped my total insulin per day from averages above 40-90+ down to the 20’s and 30’s. That change was literally overnight. As soon as I started dieting and counting carbs carefully, I no longer have to ingest extra carbs for lows because I have very little IOB now, now that I’m dieting to lose weight. So it’s a win/win. Losing weight AND better glucose control. I did this about 3-4 years ago, but fell off the wagon. I’ll be doing a happy dance when I lose another 15 lbs, because that puts me at my favorite weight.
Wow, so impressive. I’m like you, my a1c was pretty bad, 7-8 for most of my diabetic life til I started making an effort a few years ago. The OmniPod and Dexcom has really helped. I went from mid 6s to low 5s, even high 4s most recently. But unlike you, I’m very unstable with a lot of lows still. Per xdrip+, 90 day in range is 75%. I’d like that to be much higher. Std deviation is 33%. Also too high. I can do well one day but for extended time, I can’t seem to reach stable bgs for more than a day or two. So that is my focus now, try to be more stable.
Please excuse me jumping into the conversation. Your current blood glucose control is good. Your BG variability at 33 mg/dL standard deviation is also good. If I were you, I would target trying to bring that number down to 25 mg/dL, if possible. For me, I could not even approach this calming of variability until I limited my dietary carbs. Some people can eat more carbs and still enjoy good variability but I could not. I try to eat less than 75 grams of carbs per day and no more than 30 at one sitting.
I also found that daily exercise, even just 20 minutes of brisk walking, provides a good reduction of variability. When I found myself leaving for walks to chop off expected post-meal spikes, I knew is was on track for good BG performance. Sustained daily exercise also led to a reduction in my total daily insulin amount.
I’ve never had an A1c in the 4’s since becoming a T1. Way to go. I get lows pretty much every day. Years ago on animal insulins with no meter, I’d freak out due to the nature of those lows that would have me panicked thanks to the rapidity and depth of the drop, the shakes, and sweats if I had been asleep. Sometimes, believe it or not, I could drop a whopping 100 points in literally 5-6 minutes (based off of the many readings I did over the years using a visually-read strip, ChemstripbG. I don’t get upset at all now when I’m low–I just deal with it calmly (but with a lot of haste if I’m very low).
Terry, my wife and I both walk frequently as well as hike for a couple hours to an altitude gain of about 900 feet (varies), round trip. My knees are the limiting factor in us making those dirt-trail hikes up the hill. They always say the knees are the first to go! Well, my pancreas went first, but the knees are bothersome too.
Now that I know I can change the AGP report parameters, if I set the high limit to 160, my TIR is of course, less, to 86.4% and a variation of 27.9%. If I look back a few weeks it won’t be quite that good.
I’ve struggled with plantar fasciitis and achilles tendonitis for most of this year. I’ve made some significant gains recently via physical therapy. Even though, with my walking pains, I could use a stationary bicycle, I just couldn’t sustain the same consistency I had with walking. I have older siblings who have had knees replaced so I may be looking at the same thing. So far my knees are OK.