My Clarity program which ties into my Dexcom G6 says my A1c score is 6.9. A recent blood test says it is 7.6. Typically the blood test is .5 above the monitor. Which is more accurate. My endo says the Dexcom is more accurate. Thoughts?
2 Likes
I just have a year experience with the G6 and one month on a T:Slim pump. During the 11 months with the G6 and doing MDI my HbA1c was pretty close to the G6. It will be a while before I get another HbA1c. My GMI is above what I was on MDI, but my time in range, standard deviation and coefficient of variation are much better. I’m interested in what the HbA1c will be.
I know, I didn’t answer your question, but this way I will see responses from my wiser and smarter brothers and sisters here.
Dexcom Clarity stopped calling their number A1C a couple years back. They now call it “GMI” for Glucose Management Indicator because while there is an intended relationship between GMI and A1C they only agree at the +/- 1 level in real life.
Why? Because while there is a relationship between A1C and average glucose, there is a LOT of scatter in the data. The scatter plot below (from lab measurements) shows that two people with the same average glucose of 150, may have lab A1C’s that range from 5.8 to 7.9. The “A1C calculator” will say bg=150 means A1C=6.9 which is that straight line, but it doen’t do a good job representing the many reasons for scatter in the relationship.
(Note - corrected the acronym to GMI due to several pointing out how I chose the wrong TLA!)

2 Likes
The Dexcom is not more accurate. It seems to work best if you go by your average BG level versus the GMI number they use. But just think of the times you finger stick and compare with the Dexcom and how much the Dexcoms numbers are off by. So if your numbers are off, the average BG number will be off too. I usually calibrate mine to be within 5 points so my average Bg level is usually pretty spot on to what my A1C will be. But my GMI number still is almost a half point higher than my A1c always is.
But given that, the Dexcom is better at judging how you are doing overall. You can have a great looking A1c and get that by having a bunch of lows and a bunch of highs and it averages out to “look” like a good A1c. The Dexcom will tell you TIR which is a much more accurate way to tell how you are doing. And maybe that’s what your endo means.
3 Likes
The new new term is GMI, glucose management indicator.
Explanation on variations.
In my experience, I had an A1C taken while I was having chemo treatments. Lowest ever, 4.6. Based on cgm, should have been around 5.8.
Chemo reduces RBC lifespan, causing this result.
Shorter lifespan, less time to “glycate”.
1 Like
I created a topic way back regarding a study on accuracy, so not my personal results, but reposted here for ease of access:
Clarifying a bit, since it’s dense…
Term
- GMI: glucose management indicator estimates A1c from meter readings
Real-Time (rtCGM)
- CareLink Pro/Personal, Dexcom G5
- Symmetric variance of GMI around A1c
Intermittent Scanning (iscCGM)
- FreeStyle Libre
- Higher GMI compared to actual on 75% of users
Generally
- About 50% had differences between GMI and A1c of >0.5%
- Similar patterns were observed regardless of weight or age
- With average A1C < 7.5, GMI was higher than actual, more often in isCGM
- With average A1C > 7.5, A1c was higher than GMI, more often in rtCGM
- With average A1C > 7.5, isCGM was generally accurate
Synopsis
- If you have good control, you can trust your Dexcom or CareLink, but your Freestyle might be overestimating average A1c.
- An alternative assessment might turn up that the pattern of scanning by FreeStyle users is different, and they more often scan when they are high, but not when they are low.
- If you have poor control, the real-time CGM is possibly underestimating your A1c.
Study is here: https://care.diabetesjournals.org/content/43/9/e111
Personally, my Dexcom result is higher than my HbA1c result, but both are within the range of good control, but I tend to trust the CGM the most.
What is TIR?
TIR = Time-in-Range. Generally, good TIR is more important for well-being than an average over time, since it is the time over the edge, either too high or too low, that are most harmful. A good average with large excursions is poor control.
My endo likes to see 70% TIR, but I have seen studies showing a TIR of 80% is the point to aim for, and higher TIR is better than lower.
James, what does your endo say about standard deviation?
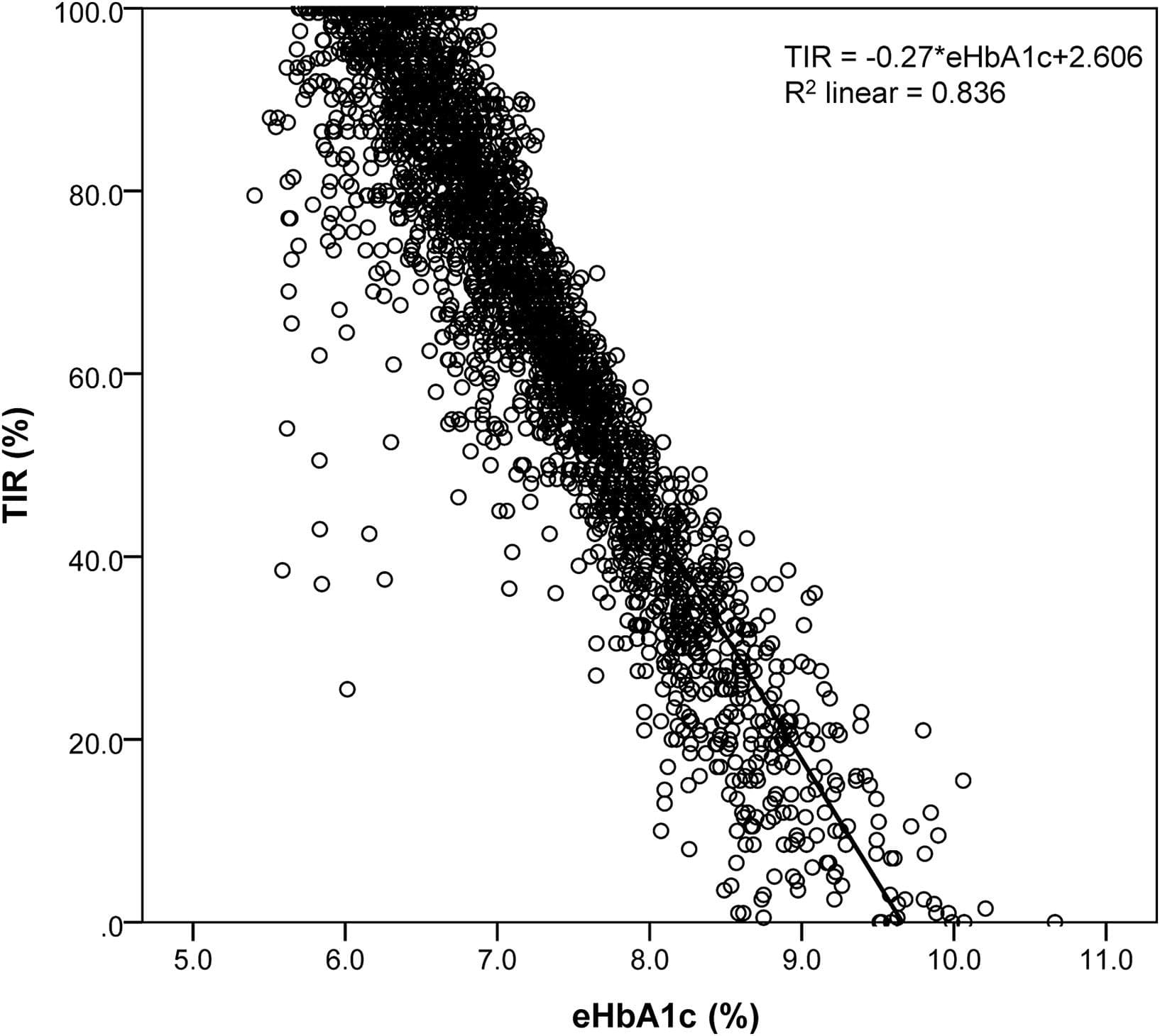
Speaking of TIR, here’s a randomly chosen scatter graph of average bg (expressed as “eHbA1c”) vs TIR in T2’s wearing CGM’s (note that their control is often much better than diabetics at large, my idea is that T2’s wearing CGM’s are those with plenty of resources who make a lot of effort. I’ve seen very different looking scatter plots of TIR vs A1C for T1’s).
This has been my general experience as well. However, the last time the Dex estimated 6.1 and my A1c was 6.2. I understand the 2-6 weeks just prior to the blood draw can make a big difference so if I have had issues with my pump or other had other difficulties staying in range during that time frame, the difference between the two measures is greater.
She hasn’t. I have seen one study that looked at, or included, standard deviation, but I’ll have to search for that. In that, the best SD was even less than 40, maybe 35, and even possibly 30, but that is a bit extreme.
TIR Time in range. Generally endos pick the numbers 70-180 as being in good control. I believe they want you in those numbers at least 70% of the time. But TIR can vary if you pick different numbers. So just people saying they are TIR 70% doesn’t mean they are 70% TIR between 70-180. So my TIR preference is usually 65-160, or 65-140. So it can vary, but I’m pretty sure endos generally use 70-180. A lot of us on this board aim for tighter TIR’s than our endos. That would be a personal choice.
Generally endos don’t like low numbers, so they don’t want to see an A1c that was derived from having high highs and low lows. The roller coaster ride sort of explains that. It is also thought that more damage is done from repeated drastic changes. So looking at TIR tells them what your numbers are actually doing. That would also be where SD comes into play (standard deviation). The amount you likely can change in your BG level. So an average change of 50 isn’t as good as an average change of 25. Plus if you hit lower numbers and you have a higher SD, it means you are more likely to drop to a “too low” number. That helps decide what average BG level to aim for.
2 Likes
I am getting my first weekly clarity reports. My average glucose level was 95, TIR 98 and standard deviation 20. No, very highs or very lows, no highs, 2% low. MDI with about 265 healthy carbs.
I am wondering what an average deviation is. I don’t have an endo and I am sure my GP wouldn’t know.
I used the range 60-160, although last week, I stayed mostly under 140-150.
I would post this, just to show that Mastering Diabetes works, but I am technically challenged and can’t figure out how to post an email from my IPad. My husband made his living as a computer technologist and he can’t figure my IPad out either. He hates Apple products.
2 Likes
Don’t forget that your A1C easily has + or - 0.5% variation between labs which is why you always want to get your A1C from the same lab. Large hospitals and clinics have equipment that is calibrated and certified and has great accuracy, however, many doctor offices have small non-certified machines and therefore A1C can vary up to 1% between 2 such offices.
@Marilyn6 Interesting question. I haven’t heard of an average SD number. I believe they want it under 30, though I could be wrong about that. 20 is great control, I know mine is usually around 22. .
1 Like
Marie, while it is theoretically possible to have an SD of 20 and an average bg of 240, that’s not very often the case.
If your work very hard and keep your bgs 70-130 most of the time, that’s the most likely way we would end up with SD’s in the 20’s.
1 Like
That could be true lol at @Tim12. But that literally would mean most of your numbers would have to fall 220-260?
I think the data from the Dexcom gives you a fuller representation of your blood glucose health. As others have said, the A1c is just an average and can hide glucose extremes. A1c accuracy can also be confounded by variation in red blood cell lifespan and iron deficiency anemia to name a few.
If the Dexcom CGM is well calibrated, it can be close to the actual blood sugar. Reporting data every five minutes gives you a much more comprehensive view of your glucose management. A high percentage time in range means fewer hypos and hypers, both good things.
Clinicians have standardized the target range as 70-180 mg/dL. They set that range for the full population of diabetics and I believe they wanted that range to be attainable for most of us.
But 70-180 is not normal for metabolically healthy non-diabetics. It represents a “reach goal” for many of us. If you can hit 90+% TIR 70-180, I would encourage you to consider lowering that upper number to a lower level. [Edited to add: in the spirit of this advice, I just lowered my upper timer range number from 130 to 120.]
I set my range at 65-130 mg/dL and can usually hit 90% with urgent lows held to less than 1%. The Dexcom CGM allows me to monitor my glycemia every day instead of the single snapshot A1c number every 90 days. For someone who uses a CGM, I think the A1c becomes irrelevant.
2 Likes